
HEALTHCARE COST AND UTLIZATION PROJECT – HCUP
A FEDERAL-STATE-INDUSTRY PARTNERSHIP IN HEALTH DATA
Sponsored by the Agency for Healthcare Research and Quality
INTRODUCTION TO
THE HCUP NATIONWIDE EMERGENCY DEPARTMENT SAMPLE (NEDS)
2007
(Version 1)
| These pages provide introductory-level information about the NEDS. For full documentation and notification of changes, visit the HCUP User Support (HCUP-US) Website at http://www.hcup-us.ahrq.gov. |
Issued January 2010
Agency for Healthcare Research and Quality
Healthcare Cost and Utilization Project (HCUP)
Phone: (866) 290-HCUP (4287)
E-mail: hcup@ahrq.gov
Website: http://www.hcup-us.ahrq.gov
NEDS Data and Documentation Distributed by:
HCUP Central Distributor
Phone: (866) 556-4287 (toll-free)
Fax: (866) 792-5313
E-mail: HCUPDistributor@ahrq.gov
Table of Contents
Skip Table of Contents
HCUP EMERGENCY DEPARTMENT SAMPLE (NEDS)
|
|
***** REMINDER ***** |
All users of the NEDS must complete the on-line Data Use Agreement (DUA) training, sign a Data Use Agreement, and send a copy to AHRQ.† Authorized users of HCUP data agree to the following limitations: ‡
Any violation of the limitations in the Data Use Agreement is punishable under Federal law by a fine of up to $10,000 and up to 5 years in prison. Violations may also be subject to penalties under State statutes. |
† The on-line Data Use Agreement training session and the Data Use Agreement are available on the HCUP User Support (HCUP-US) Website at http://www.hcup-us.ahrq.gov. |
HCUP CONTACT INFORMATION
The NEDS Data Use Agreement Training Tool and the Data Use Agreement are available on the AHRQ-sponsored HCUP User Support (HCUP-US) Website:
After completing the on-line training, please submit signed Data Use Agreements to HCUP at:
For technical assistance:
|
WHAT IS THE NATIONWIDE EMERGENCY DEPARTMENT SAMPLE (NEDS)?
|
|
|
UNDERSTANDING THE NEDS
|
|
HEALTHCARE COST AND UTILIZATION PROJECT — HCUP
A FEDERAL-STATE-INDUSTRY PARTNERSHIP IN HEALTH DATA
Sponsored by the Agency for Healthcare Research and Quality
HCUP Nationwide Emergency Department Sample (NEDS)
ABSTRACT
The Nationwide Emergency Department Sample (NEDS) is part of the Healthcare Cost and Utilization Project (HCUP), sponsored by the Agency for Healthcare Research and Quality (AHRQ). The 2007 NEDS is a publicly available database that can be purchased through the HCUP Central Distributor.
The NEDS was created to enable analyses of emergency department (ED) utilization patterns and support public health professionals, administrators, policymakers, and clinicians in their decision-making regarding this critical source of care. The ED serves a dual role in the U.S. healthcare system infrastructure as a point of entry for approximately 50% of inpatient hospital admissions and as a setting for treat-and-release outpatient visits 1 The NEDS has many research applications, as it contains information about geographic characteristics, hospital characteristics, patient characteristics, and the nature of visits (e.g., common reasons for ED visits, including injuries).
The NEDS is the largest all-payer ED database that is publicly available in the United States, containing information from about 27 million ED visits at about 970 hospitals that approximate a 20-percent stratified sample of U.S. hospital-based EDs. Weights are provided to calculate national estimates pertaining to over 120 million ED visits in 2007.
The NEDS is drawn from States that provide HCUP with ED data (resulting in admission to the hospital and not). Twenty-seven HCUP States participated in the 2007 NEDS: AZ, CA, CT, FL, GA, HI, IA, IN, KS, MA, MD, ME, MN, MO, NC, NE, NH, NJ, NY, OH, RI, SC, SD, TN, UT, VT, and WI. See Appendix I, Table 1 for a list of data organizations participating in the NEDS.
By stratifying on important hospital characteristics, the NEDS represents a microcosm of U.S. hospital-based EDs. Stratification is based on the following five characteristics:
Access to the NEDS is open to users who sign Data Use Agreements. Uses are limited to research and aggregate statistical reporting.
For more information on the NEDS, visit the AHRQ-sponsored HCUP User Support (HCUP-US) Website at http://www.hcup-us.ahrq.gov.
INTRODUCTION TO THE HCUP NATIONWIDE EMERGENCY DEPARTMENT SAMPLE (NEDS)
Overview of NEDS Data
The Healthcare Cost and Utilization Project (HCUP) Nationwide Emergency Department Sample (NEDS) was created to enable analyses of emergency department (ED) utilization patterns and support public health professionals, administrators, policymakers, and clinicians in their decision-making regarding this critical source of care. The ED serves a dual role in the U.S. healthcare system infrastructure as a point of entry for approximately 50% of inpatient hospital admissions and as a setting for treat-and-release outpatient visits.2 The NEDS has many research applications, as it contains information about geographic characteristics, hospital characteristics, patient characteristics, and the nature of visits (e.g., common reasons for ED visits, acute and chronic conditions, and injuries).
Twenty-seven States participated in the 2007 NEDS. These States include: AZ, CA, CT, FL, GA, HI, IA, IN, KS, MA, MD, ME, MN, MO, NC, NE, NH, NJ, NY, OH, RI, SC, SD, TN, UT, VT, and WI. Appendix I, Table 1 identifies the specific data organizations contributing to the NEDS.
Appendix 1, Figure 1represents the geographic distribution of the 27 participating HCUP Partner States. Based on 2007 U.S. Census Bureau data, the HCUP NEDS States account for 61.3% of the U.S. population. The 27 States account for 59.6% of the ED visits reported in the 2007 American Hospital Association (AHA) Annual Survey Database. Details on the percentage of population and ED visits by region are provided in Appendix I, Table 2.
Identification of HCUP Records with Emergency Department Services
Information on patients with ED events are contained in two existing HCUP databases:
Both of these HCUP databases contain a core set of clinical and non-clinical information elements defined in a uniform scheme for all patients, regardless of payer, making it possible to combine records across databases.
Selection of ED records from the SEDD and SID for use in the NEDS was based on evidence of ED services reported on the record. The HCUP criteria for identifying an ED record (i.e., a discharge record for a patient with an ED event) require that at least one of the following conditions is true:
Because six of the 27 Partners (AZ, CA, HI, MA, NC, and OH) did not provide ED charge information (either in revenue codes or a separate charge field) on records in the SEDD, this limited the ability to clearly identify ED visits using the HCUP criteria. Therefore, the identification of ED records in these States was evaluated on a State-by-State basis.
State-Specific Restrictions
Some sources that contributed data to the NEDS imposed restrictions on the release of certain data elements or on the number and types of hospitals that could be included in the database. In addition, because of confidentiality laws, some data sources were prohibited from providing HCUP with discharge records that indicated specific medical conditions, such as HIV/AIDS or behavioral health. Detailed information on these State-specific restrictions is available in Appendix II.
File Structure of the NEDS
Because of the size of the NEDS and the difference in information collected on records for patients admitted into the hospital directly from the ED (SID records) and for ED patients that are not admitted (SEDD records), the NEDS is divided into four different files:
NEDS Data Elements
The coding of data elements in the NEDS is consistent with other HCUP databases. The following three objectives guided the definition of data elements in all HCUP databases:
More information on the coding of HCUP data elements is available on HCUP User Support (HCUP-US) Website (http://www.hcup-us.ahrq.gov/db/coding.jsp).
After analyzing the availability of information from the HCUP Partner States, a set of common fields to be available in the NEDS was created. The NEDS contains more than 100 clinical and non-clinical variables provided in a hospital discharge abstract, such as:
Appendix III identifies the data elements in each NEDS file:
Not all data elements in the NEDS are uniformly coded or available across all States. The tables in Appendix III provide summary documentation for the data. Please refer to the NEDS documentation located on the HCUP-US Website (http://www.hcup-us.ahrq.gov) for comprehensive information about data elements and the files.
Getting Started
Comprehensive documentation for the NEDS files is available on the HCUP-US Website (http://hcup-us.ahrq.gov).
NEDS Data Files
The 2007 NEDS is a publicly available database that can be purchased through the HCUP Central Distributor. Contact the HCUP Central Distributor with questions about the NEDS and to purchase your own copy.
NEDS Documentation
On the HCUP-US Website (http://www.hcup-us.ahrq.gov), users of the NEDS can access complete file documentation, including variable notes, file layouts, summary statistics, and related technical reports. Similarly, data users can download SAS, SPSS, and Stata load programs. Refer to these important resources to understand the structure and content of the NEDS and to aid in using the database.
To locate the NEDS documentation on HCUP-US:
Appendix 1, Table 3 details the comprehensive NEDS documentation available on HCUP-US.
SAMPLING DESIGN OF THE NEDS
Similar to the design of the Nationwide Inpatient Sample (NIS), the NEDS is built using a 20% stratified sample of institutions. For the NIS, it is a sample of U.S. hospitals. For the NEDS, it is a sample of U.S. hospital-based EDs. The main objective of a stratified sample is to ensure that the sample is representative of the target universe. By stratifying on important hospital characteristics, the NEDS represents a "microcosm" of EDs in the U.S. For example, by including trauma center designation in the sampling strategy, the NEDS has the same percentage of trauma hospitals as the entire U.S. The NEDS contains all of the ED visits for the sample of hospital-based EDs selected.
Universe of Hospital-Based Emergency Departments
A feasibility study performed in 2008 assessed several possible data sources for the universe of hospital-based EDs in the United States: the American Hospital Association (AHA) Annual Survey Database (Health Forum, LLC © 2012); Verispan, LLC databases (now called SDI Health LLC); and the Centers for Medicare and Medicaid (CMS) Hospital Cost Reports. The AHA Annual Survey Database is the best data to apply for a number of reasons. First, the AHA data provides the necessary hospital characteristics, such as ownership type and teaching status, and also reports total ED visits for hospitals. Second, the crosswalk linkage from the HCUP databases to the AHA data is already established. Third, the AHA Annual Survey Database is used as the target universe for the NIS. The universe of hospital-based EDs is therefore defined as AHA community, non-rehabilitation hospitals that reported total ED visits. The AHA defines community hospitals as "all non-Federal, short-term, general, and other specialty hospitals."
Sampling Frame of the NEDS
The sampling frame of the NEDS is limited to a subset of the universe: hospital-based EDs in the States for which HCUP ED data (SID and SEDD) are available. The list of hospital-based EDs in the frame consists of all AHA community, non-rehabilitation hospitals that report total ED visits in each of the frame States that could be matched to the ED data provided to HCUP. If an ED in the AHA survey could not be matched to the ED data provided by the HCUP data source, it is eliminated from the sampling frame (but not from the target universe).
Stratification Variables
The following hospital characteristics were used for sample stratification: U.S. Census region, trauma center designation, urban-rural location of the hospital, ownership, and teaching status. ED bed size was not used because no data source for this information could be identified. A number of data sources report the bed size of the hospital, but no source distinguishes between inpatient and ED beds.
The NEDS stratification variables are described below and detailed in Appendix I, Table 5.
U.S. Census Region
The four Census regions – Northeast, Midwest, South, and West – were used to stratify EDs by geographic location because practice patterns may vary substantially by region. Appendix I, Figure 1 shows the NEDS States by region.
Trauma Centers
A trauma center is a hospital equipped to provide comprehensive emergency medical services 24 hours a day, 365 days per year to patients suffering traumatic injuries. For the NEDS, trauma centers were identified through the Trauma Information Exchange Program database (TIEP), a national inventory of trauma centers in the U.S. Information is collected by the American Trauma Society and the Johns Hopkins Center for Injury Research and Policy and funded by the Centers for Disease Control and Prevention.3,4
The TIEP database is updated quarterly and identifies all U.S. hospitals that are designated as trauma centers by a State or regional authority or verified by the American College of Surgeons' Committee on Trauma (ACS/COT). Designation of trauma center levels I, II, and III are based on criteria developed by the ACS/COT. Level I and II centers have comprehensive resources and are able to care for the most severely injured. Level I centers also provide leadership in education and research. Level III centers provide prompt assessment and resuscitation, emergency surgery and, if needed, transfer to a level I or II center. Level IV and V centers are State-defined and often located in remote areas. These centers resuscitate and stabilize patients and arrange transfer to an appropriate trauma facility. For the NEDS, levels I, II and III were used to identify a trauma center. Level IV and V centers were set aside within the context of these data because many states choose not to designate hospitals at these levels of trauma care and their institutional characteristics have many similarities to community (non-trauma) hospitals in other areas. It is also important to note that while all level I, II, and III trauma centers offer a high level of trauma care, that there may be differences in the services and resources offered by hospitals of different levels. Further, hospitals of different levels may be utilized in diverse ways within the context of individual state trauma systems or the geographic areas in which they operate.
Hospital information from TIEP was matched to the AHA via the corresponding AHA hospital identifier and then added to the HCUP ED data. If the trauma level of a hospital changed during the calendar year, the highest trauma level (indicating the lowest level of care) was used. For example, if a hospital-based ED was reported as trauma level II for two quarters of 2007 and trauma level III for two quarters of 2007, then the hospital-based ED was considered a level III trauma center for the 2007 NEDS. Alternatively, if a hospital-based ED was reported as a trauma level III for 2 quarters of 2007 and did not report for two quarters, the ED was considered a trauma level III for the 2007 NEDS.
In the 2007 NEDS, trauma centers that are level I, II, and III are distinguished. If the strata size in the universe or frame was less than two hospitals, a collapsed stratification of levels I and II or levels I, II, and III was necessary.
Urban-Rural Location of the ED
The urban-rural location of hospital-based EDs was determined based on the county in which the hospital is located. The categorization is a simplified adaptation of the 2003 version of the Urban Influence Codes (UIC). 5 The 12 categories of the UIC are combined into four broader categories:
If the strata size in the universe or frame was less than two hospitals, a collapsed stratification of metropolitan (large and small) or non-metropolitan (micropolitan and non-urban residual) was necessary.
Teaching Status
A hospital-based ED is considered to be a teaching facility if the associated hospital has an American Medical Association (AMA) approved residency program, is a member of the Council of Teaching Hospitals (COTH), or has a ratio of full-time equivalent interns and residents to beds of 0.25 or higher according to the AHA Annual Survey Database. Because there are very few teaching hospitals in micropolitan and rural areas, teaching status was only used to stratify EDs in metropolitan areas.
Hospital Ownership
Hospital ownership or control was categorized according to information reported in the AHA Annual Survey Database. Ownership categories include:
When there were enough hospitals of each type, EDs were stratified into public, voluntary, and proprietary categories. If necessary, because of small strata size in the universe, a collapsed stratification of public versus private was used, with the voluntary, non-profit and proprietary/ for-profit hospitals combined to form a single "private" category. Stratification based on ownership or control was not advisable in some regions because of the dominance of one type of hospital (e.g., Northeast).
Sample Weights
To obtain nationwide estimates, weights were developed using the AHA universe as the standard. These were developed separately for analyses of hospital-based EDs and ED visits. Hospital-level weights were developed to extrapolate NEDS sample EDs to the universe of hospital-based EDs. Similarly, discharge-level discharge weights were developed to extrapolate NEDS sample ED visits to the universe of ED visits.
Hospital Weights
Hospital weights to the universe were calculated by poststratification. Hospital-based EDs were stratified on the same variables that were used for sampling: geographic region, trauma center designation, urban-rural location, teaching status, and ownership or control. The strata that were collapsed for sampling were also collapsed for sample weight calculations. Within each stratum, s, each ED in the NEDS sample received a weight:
Discharge Weights
Discharge weights to the universe were calculated by poststratification. Hospital-based EDs were stratified in a manner similar to that for universe hospital weight calculations. Within stratum, s, for hospital, i, the universe weight for each visit in the NEDS sample was calculated as:
Final NEDS Sample
The target universe for the NEDS was community, non-rehabilitation hospitals in the United States that were included in the 2007 AHA Annual Survey Database and reported total ED visits. Excluded were a handful of non-rural hospitals that reported less than 10 ED visits in a year.
The NEDS sampling frame included hospital-based ED events from community, non-rehabilitation hospitals in the 27 HCUP Partner States that provide discharge abstracts on patients admitted to the hospital through the ED and patients treated and released or transferred to another hospital from the ED. The HCUP hospitals were required to be represented in the AHA data and have no more than 90% of their ED visits resulting in admission. Appendix I, Table 6 lists the final target universe and sampling frame for the NEDS.
The NEDS is a stratified probability sample of hospital-based EDs in the frame, with sampling probabilities calculated to select 20% of the universe contained in each stratum, defined by region, trauma designation, urban-rural location, teaching status, and hospital ownership or control. A sample size of 20 percent was based on previous experience with similar research databases. A larger sample would be cumbersome for data users given that a 20% sample contains over 25 million records. A 20% sample also enables the user to split the NEDS into two 10% subsamples for estimation and validation of models.
To further ensure accurate geographic representation, hospitals were implicitly stratified by State and three-digit ZIP Code (i.e., the first three digits of the hospital's five-digit ZIP Code). This was accomplished by sorting by three-digit ZIP Code within each stratum prior to drawing a systematic random sample of hospitals. Within the three-digit ZIP Code, hospitals were sorted by a random number to ensure further geographic generalizability of hospitals within the frame States; otherwise, generally, three-digit ZIP Codes that are proximal in value are geographically near one another within a State. Furthermore, the U.S. Postal Service locates regional mail distribution centers at the three-digit level. Thus, the boundaries tend to be a compromise between geographic size and population size.
Using the universe of U.S. hospital-based EDs, strata were defined by region, trauma designation, urban-rural location, teaching status, and hospital ownership or control. Strata with less than two hospitals in the universe and frame were collapsed with adjacent stratum based on urban-rural location, trauma designation, or ownership or control.
After stratifying and sorting the universe of hospitals, a random sample of up to 20% of the total number of hospital-based EDs in the U.S. was selected within each stratum. A shortfall was defined as an insufficient number of EDs in the frame to meet the threshold of 20% of the universe. In strata with shortfalls, the sampling rate from the universe was less than 20% and all possible EDs in the frame are selected for the NEDS. In contrast, the sampling rate is larger than 20% in some strata because protecting hospital confidentiality required a minimum of two sampled EDs in each stratum. Appendix I, Table 7 lists the sampling rates by stratum for the NEDS.
HOW TO USE THE NEDS FOR DATA ANALYSIS
This section provides a brief synopsis of special considerations when using the NEDS. For more details, refer to the comprehensive documentation on the HCUP-US Website (http://hcup-us.ahrq.gov/).
If anyone (regardless of whether they are the original recipient of the data) uses the NEDS, be sure s/he reads and signs a Data Use Agreement after completing the on-line Data Use Agreement training available on the HCUP-US Website (http://www.hcup-us.ahrq.gov). A copy of the signed Data Use Agreements must be sent to AHRQ. See page 2 for the mailing address.
Limitations of the NEDS
The NEDS contains about 27 million ED records and over 100 clinical and non-clinical data elements. This allows for a multitude of research studies, yet there are some limitations.
Identifying Different Types of ED Events
Calculating National Estimates
Choosing Data Elements for Analysis
ICD-9-CM Diagnosis and Procedure Codes
Missing Values
Variance Calculations
It may be important for researchers to calculate a measure of precision for some estimates based on the NEDS sample data. Variance estimates must take into account both the sampling design and the form of the statistic. The sampling design consisted of a stratified, single-stage cluster sample. A stratified random sample of hospital-based EDs (clusters) was drawn and then all ED visits were included from each selected hospital. To accurately calculate variances from the NEDS, appropriate statistical software and techniques must be used. For details, see the special report Calculating Nationwide Inpatient Sample Variances on the HCUP-US Website (www.hcup-us.ahrq.gov). The NIS uses the same stratified sample design, so techniques appropriate for the NIS are also appropriate for the NEDS.
If hospitals inside the sampling frame are similar to hospitals outside the frame, the sample hospitals can be treated as if they were randomly selected from the entire universe of hospitals within each stratum. Standard formulas for a stratified, single-stage cluster sample without replacement could be used to calculate statistics and their variances in most applications.
A multitude of statistics can be estimated from the NEDS data. Several computer programs that calculate statistics and their variances from sample survey data are listed in the next section. Some of these programs use general methods of variance calculations (e.g., the jackknife and balanced half-sample replications) that take into account the sampling design. However, it may be desirable to calculate variances using formulas specifically developed for certain statistics.
These variance calculations are based on finite-sample theory, which is an appropriate method for obtaining cross-sectional, nationwide estimates of outcomes. According to finite-sample theory, the intent of the estimation process is to obtain estimates that are precise representations of the nationwide population at a specific point in time. In the context of the NEDS, any estimates that attempt to accurately describe characteristics and interrelationships among hospitals and ED visits during a specific year should be governed by finite-sample theory. Examples would be estimates of expenditure and utilization patterns.
Alternatively, in the study of hypothetical population outcomes not limited to a specific point in time, the concept of a "superpopulation" may be useful. Analysts may be less interested in specific characteristics of the finite population (and time period) from which the sample was drawn than they are in hypothetical characteristics of a conceptual superpopulation from which any particular finite population in a given year might have been drawn. According to this superpopulation model, the nationwide population in a given year is only a snapshot in time of the possible interrelationships among hospital, market, and discharge characteristics. In a given year, all possible interactions between such characteristics may not have been observed, but analysts may wish to predict or simulate interrelationships that may occur in the future.
Under the finite-population model, the variances of estimates approach zero as the sampling fraction approaches one. This is the case because the population is defined at that point in time and because the estimate is for a characteristic as it existed when sampled. This is in contrast to the superpopulation model, which adopts a stochastic viewpoint rather than a deterministic viewpoint. That is, the nationwide population in a particular year is viewed as a random sample of some underlying superpopulation over time. Different methods are used for calculating variances under the two sample theories. The choice of an appropriate method for calculating variances for nationwide estimates depends on the type of measure and the intent of the estimation process.
Computer Software for Weighted and Variance Calculations
The hospital weights are useful for producing hospital-level statistics for analyses that use the hospital-based ED as the unit of analysis. In contrast, the discharge weights are useful for producing visit-level statistics for analyses that use the ED visit as the unit of analysis.
In most cases, computer programs are readily available to perform these calculations. Several statistical programming packages allow weighted analyses.6 For example, nearly all SAS procedures incorporate weights. In addition, several statistical analysis programs have been developed to specifically calculate statistics and their standard errors from survey data. Version 8 or later of SAS contains procedures (PROC SURVEYMEANS and PROC SURVEYREG) for calculating statistics based on specific sampling designs. STATA and SUDAAN are two other common statistical software packages that perform calculations for numerous statistics arising from the stratified, single-stage cluster sampling design. Examples of the use of SAS, SUDAAN, and STATA to calculate NIS variances are presented in the special report Calculating Nationwide Inpatient Sample Variances on the HCUP-US Website (www.hcup-us.ahrq.gov). While the examples using the NIS also apply to the NEDS, it should be noted that the NEDS is a much larger data set. Please consult the documentation for the different software packages concerning the use of large databases. For an excellent review of programs to calculate statistics from survey data, visit the following website: http://www.hcp.med.harvard.edu/statistics/survey-soft/. ![]()
The NEDS includes a Hospital Weights File with variables required by these programs to calculate finite-population statistics. The file includes synthetic hospital identifiers (Primary Sampling Units or PSUs), stratification variables, and stratum-specific totals for the numbers of ED visits and hospitals so that finite-population corrections can be applied to variance estimates.
In addition to these subroutines, standard errors can be estimated by validation and cross-validation techniques. Given that a very large number of observations will be available for most NEDS analyses, it may be feasible to set aside a part of the data for validation purposes. Standard errors and confidence intervals then can be calculated from the validation data.
If the analytic file is too small to set aside a large validation sample, cross-validation techniques may be used. For example, ten-fold cross-validation would split the data into ten subsets of equal size. The estimation would take place in ten iterations. In each iteration, the outcome of interest is predicted for one-tenth of the observations by an estimate based on a model fit to the other nine-tenths of the observations. Unbiased estimates of error variance are then obtained by comparing the actual values to the predicted values obtained in this manner.
COMPARABLE ED DATA SOURCES
To aid in understanding of NEDS, national estimates from the NEDS are compared to available sources of similar data. Each of the following ED data sources has potential for use in research addressing ED utilization and policy and has data available for 2007.
| Type of ED Data | ED Data Source | Description |
|---|---|---|
| National inventories of hospital-based EDs | American Hospital Association Annual Survey of Hospitals (AHA) | Database containing characteristics and descriptions of U.S. hospitals reported by hospitals via survey. Sponsored by American Hospital Association. |
| National Emergency Department Inventory (NEDI) - USA | Inventory of U.S. ED locations and annual ED visit volume which integrates information from the AHA Annual Survey, the Hospital Market Profiling Solution©, Internet searches, and direct communication with hospital staff. Created by the Emergency Medicine Network (EMNet). | |
| ED visit information from a sample of hospital-based EDs | HCUP Nationwide Emergency Department Sample (NEDS) | Nationwide sample drawn from the HCUP SID and SEDD, stratified and weighted to be nationally representative of ED visits and facilities. Sponsored by the Agency for Healthcare Research and Quality (AHRQ) of the U.S. Department of Health and Human Services (DHHS). |
| National Hospital Ambulatory Medical Care Survey (NHAMCS) | National probability sample survey of utilization and provision of ambulatory services in hospital emergency and outpatient departments. Sponsored by National Center for Health Statistics (NCHS) of the DHHS' Centers for Disease Control and Prevention (CDC). | |
| National Electronic Injury Surveillance System - All Injury Program (NEISS-AIP) | National probability sample providing counts of injuries seen in the ED. Sponsored by National Center for Injury Prevention and Control (NCIPC) of the DHHS' CDC and US Consumer Product Safety Commission (CPSC). | |
| ED visit information from a sample of patients | National Health Interview Survey (NHIS) | A comprehensive survey of the civilian noninstitutionalized population residing in the United States at the time of the interview. Sponsored by National Center for Health Statistics (NCHS) of the DHHS' CDC. |
Information on total ED visits in 2007 for the U.S. was available from five data sources (AHA, NEDS, NEDI, NHAMCS, and NHIS). Appendix IV, Figure 1 displays the range of total ED visits; Appendix IV, Table 1 lists the total ED visits in the U.S and by census region. Total U.S. ED visit counts are relatively consistent across the data sources. The South consistently has the highest number of ED visits and the West had the lowest number of ED visits.
Information on the total number of ED visits by region and the percentage of all ED visits resulting in inpatient admissions are available from two data sources (NHAMCS and NEDS) and are displayed in Appendix IV, Table 2.
Estimates of the number of hospital-based EDs by ED visit volume are available from three data sources (NEDS, AHA, and NEDI) and are displayed in Appendix IV, Table 3.
Estimates of the number of injury-related ED visits are available from three data sources (NEDS, NHAMCS, and NEISS-AIP) and are displayed in Appendix IV, Table 4.
Appendix I: NEDS Introductory Information
Table 1. HCUP Partners Participating in the 2007 NEDS
| State | HCUP Data Source |
|---|---|
| Arizona | Arizona Department of Health Services |
| California | Office of Statewide Health Planning and Development |
| Connecticut | Connecticut Hospital Association |
| Florida | Florida Agency for Health Care Administration |
| Georgia | Georgia Hospital Association |
| Hawaii | Hawaii Health Information Corporation |
| Indiana | Indiana Hospital&Health Association |
| Iowa | Iowa Hospital Association |
| Kansas | Kansas Hospital Association |
| Maine | Maine Health Data Organization |
| Maryland | Health Services Cost Review Commission |
| Massachusetts | Division of Health Care Finance and Policy |
| Minnesota | Minnesota Hospital Association |
| Missouri | Hospital Industry Data Institute |
| Nebraska | Nebraska Hospital Association |
| New Hampshire | New Hampshire Department of Health & Human Services |
| New Jersey | New Jersey Department of Health and Senior Services |
| New York | New York State Department of Health |
| North Carolina | North Carolina Department of Health and Human Services |
| Ohio | Ohio Hospital Association |
| Rhode Island | Rhode Island Department of Health |
| South Carolina | South Carolina State Budget & Control Board |
| South Dakota | South Dakota Association of Healthcare Organizations |
| Tennessee | Tennessee Hospital Association |
| Utah | Office of Health Care Statistics, Utah Department of Health |
| Vermont | Vermont Association of Hospitals and Health Systems |
| Wisconsin | Wisconsin Department of Health Services |
Figure 1. HCUP States Participating in the 2007 NEDS
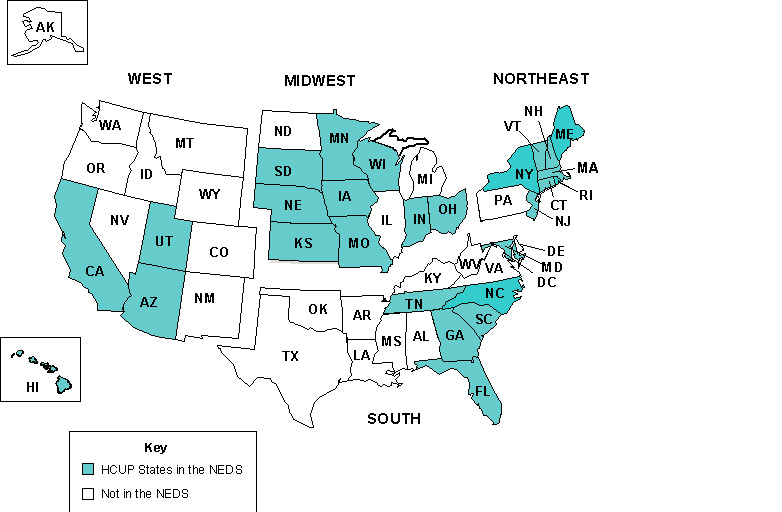
Table 2. Percentage of U.S Population and AHA ED Visits Accounted for by the 27 HCUP States Participating in the NEDS, 2007
| Region | U.S. Population in HCUP ED States | Percentage of U.S. Population in HCUP ED States (%) | AHA ED Visits in HCUP ED States | Percentage of AHA ED Visits in HCUP ED States (%) |
|---|---|---|---|---|
| Northeast | 42,341,763 | 77.3 | 18,154,250 | 75.7 |
| Midwest | 42,799,059 | 64.5 | 18,811,428 | 65.5 |
| South | 52,937,346 | 48.0 | 22,503,343 | 46.8 |
| West | 46,677,236 | 66.8 | 13,489,908 | 62.5 |
| Nation | 184,755,404 | 61.3 | 72,958,929 | 59.6 |
Restrictions on the Use of the NEDS
|
Load Programs
Programs to load the ASCII data files into statistical software:
|
|
Description of the NEDS Files
|
HCUP Tools: Labels and Formats
|
|
Description of Data Elements in the NEDS
|
NEDS-Related Reports
|
| ED Event | Number of ED Visits | Percent of ED Visits |
|---|---|---|
| ED visit in which the patient is treated and released | 99,069,433 | 81.0 |
| ED visit in which the patient is admitted to this same hospital | 19,066,478 | 15.6 |
| ED visit in which the patient is transferred to another short-term hospital | 1,385,010 | 1.1 |
| ED visit in which the patient died in the ED | 190,020 | 0.2 |
| ED visit in which patient is not admitted to this same hospital, destination unknown | 2,613,898 | 2.1 |
| ED visit in which the patient is discharged alive, destination unknown (but not admitted) | 6,900 | 0.0 |
| Stratifier | Values |
|---|---|
| Region | 1: Northeast 2: Midwest 3: South 4: West |
| Trauma | 0: Not a trauma center 1: Trauma center level I 2: Trauma center level II 3: Trauma center level III Collapsed categories used for strata with small sample sizes 8: Trauma center level I or II 9: Trauma center level I, II or III |
| Urban-Rural | 1: Large metropolitan 2: Small metropolitan 3: Micropolitan 4: Non-urban residual Collapsed categories used for strata with small sample sizes 8: Metropolitan (large and small) 9: Non-metropolitan (micropolitan and non-urban location) |
| Teaching | 0: Metropolitan non-teaching 1: Metropolitan teaching 2: Non-metropolitan teaching and non-teaching |
| Control | 0: All (used for combining public, voluntary, and private) 1: Public – government, non-Federal 2: Voluntary – private, non-profit 3: Proprietary – private, investor-owned/for-profit 4: Private (used for combining private voluntary and proprietary) |
| Description | Number of Hospital-Based EDs | Number of ED Events | |
|---|---|---|---|
| Target Universe | EDs in community, non-rehabilitation U.S. hospitals that reported total ED visits in the AHA Annual Survey Database | 4,809 | 122,331,739 |
| Sampling Frame | EDs in the 24 HCUP States that provide information on ED visits that result and do not result in admission | 2,339 | 63,925,327 |
| 2007 NEDS | 20% sample of target universe drawn from the sampling frame | 966 | 26,971,660 |
| NEDS Stratum | Number of Hospital-Based EDs | Sampling Rate | |||||
|---|---|---|---|---|---|---|---|
| NEDS Stratum | AHA Universe | 20% of Universe | Frame | Frame Shortfall | NEDS | NEDS to Universe | NEDS to Frame |
| Total | 4809 | 996 | 2339 | 30 | 966 | 20.1% | 41.3% |
| Northeast | |||||||
| 10100 | 153 | 31 | 97 | 0 | 31 | 20.3% | 32.0% |
| 10110 | 98 | 20 | 74 | 0 | 20 | 20.4% | 27.0% |
| 10200 | 103 | 21 | 65 | 0 | 21 | 20.4% | 32.3% |
| 10210 | 24 | 5 | 13 | 0 | 5 | 20.8% | 38.5% |
| 10320 | 80 | 16 | 42 | 0 | 16 | 20.0% | 38.1% |
| 10420 | 52 | 11 | 41 | 0 | 11 | 21.2% | 26.8% |
| 11110 | 41 | 9 | 730 | 0 | 9 | 22.0% | 30.0% |
| 11210 | 11 | 3 | 4 | 0 | 3 | 27.3% | 75.0% |
| 12100 | 6 | 2 | 5 | 0 | 2 | 33.3% | 40.0% |
| 12110 | 14 | 3 | 9 | 0 | 3 | 21.4% | 33.3% |
| 12200 | 10 | 2 | 7 | 0 | 2 | 20.0% | 28.6% |
| 12210 | 17 | 4 | 9 | 0 | 4 | 23.5% | 44.4% |
| 13100 | 6 | 2 | 4 | 0 | 2 | 33.3% | 50.0% |
| 13110 | 2 | 2 | 2 | 0 | 2 | 100.0% | 100.0% |
| 13920 | 7 | 2 | 6 | 0 | 2 | 28.6% | 33.3% |
| 18320 | 6 | 2 | 2 | 0 | 2 | 33.3% | 100.0% |
| Midwest | |||||||
| 20100 | 189 | 38 | 103 | 0 | 38 | 20.1% | 36.9% |
| 20110 | 65 | 13 | 32 | 0 | 13 | 20.0% | 40.6% |
| 20200 | 163 | 33 | 95 | 0 | 33 | 20.2% | 34.7% |
| 20210 | 38 | 8 | 25 | 0 | 8 | 21.1% | 32.0% |
| 20321 | 62 | 13 | 46 | 0 | 13 | 21.0% | 28.3% |
| 20324 | 172 | 35 | 111 | 0 | 35 | 20.3% | 31.5% |
| 20421 | 204 | 41 | 165 | 0 | 41 | 20.1% | 24.8% |
| 20424 | 244 | 49 | 155 | 0 | 49 | 20.1% | 31.6% |
| 21110 | 27 | 6 | 13 | 0 | 6 | 22.2% | 46.2% |
| 21210 | 21 | 5 | 11 | 0 | 5 | 23.8% | 45.5% |
| 22110 | 17 | 4 | 4 | 0 | 4 | 23.5% | 100.0% |
| 22210 | 30 | 6 | 15 | 0 | 6 | 20.0% | 40.0% |
| 22324 | 10 | 2 | 2 | 0 | 2 | 20.0% | 100.0% |
| 23100 | 17 | 4 | 14 | 0 | 4 | 23.5% | 28.6% |
| 23110 | 5 | 2 | 4 | 0 | 2 | 40.0% | 50.0% |
| 23200 | 32 | 7 | 31 | 0 | 7 | 21.9% | 22.6% |
| 23210 | 15 | 3 | 15 | 0 | 3 | 20.0% | 20.0% |
| 23321 | 4 | 2 | 2 | 0 | 2 | 50.0% | 100.0% |
| 23324 | 28 | 6 | 25 | 0 | 6 | 21.4% | 24.0% |
| 23420 | 21 | 5 | 18 | 0 | 5 | 23.8% | 27.8% |
| 28800 | 49 | 10 | 15 | 0 | 10 | 20.4% | 66.7% |
| South | |||||||
| 30101 | 41 | 9 | 16 | 0 | 9 | 22.0% | 56.3% |
| 30102 | 157 | 32 | 75 | 0 | 32 | 20.4% | 42.7% |
| 30103 | 181 | 37 | 58 | 0 | 37 | 20.4% | 63.8% |
| 30110 | 95 | 19 | 38 | 0 | 19 | 20.0% | 50.0% |
| 30201 | 81 | 17 | 31 | 0 | 17 | 21.0% | 54.8% |
| 30202 | 141 | 29 | 64 | 0 | 29 | 20.6% | 45.3% |
| 30203 | 159 | 32 | 41 | 0 | 32 | 20.1% | 78.0% |
| 30210 | 40 | 8 | 5 | 3 | 5 | 12.5% | 100.0% |
| 30321 | 80 | 16 | 26 | 0 | 16 | 20.0% | 61.5% |
| 30322 | 120 | 24 | 50 | 0 | 24 | 20.0% | 48.0% |
| 30323 | 79 | 16 | 26 | 0 | 16 | 20.3% | 61.5% |
| 30421 | 211 | 43 | 51 | 0 | 43 | 20.4% | 84.3% |
| 30422 | 184 | 37 | 42 | 0 | 37 | 20.1% | 88.1% |
| 30423 | 87 | 18 | 24 | 0 | 18 | 20.7% | 75.0% |
| 31110 | 28 | 6 | 10 | 0 | 6 | 21.4% | 60.0% |
| 31210 | 27 | 6 | 15 | 0 | 6 | 22.2% | 40.0% |
| 32110 | 9 | 2 | 4 | 0 | 2 | 22.2% | 50.0% |
| 32210 | 15 | 3 | 5 | 0 | 3 | 20.0% | 60.0% |
| 33800 | 45 | 9 | 11 | 0 | 9 | 20.0% | 81.8% |
| 33810 | 26 | 6 | 3 | 3 | 3 | 11.5% | 100.0% |
| 38800 | 22 | 5 | 4 | 1 | 4 | 18.2% | 100.0% |
| 39920 | 41 | 9 | 5 | 4 | 5 | 12.2% | 100.0% |
| West | |||||||
| 40101 | 21 | 5 | 16 | 0 | 5 | 23.8% | 31.3% |
| 40102 | 114 | 23 | 90 | 0 | 23 | 20.2% | 25.6% |
| 40103 | 78 | 16 | 54 | 0 | 16 | 20.5% | 29.6% |
| 40110 | 55 | 11 | 37 | 0 | 11 | 20.0% | 29.7% |
| 40201 | 31 | 7 | 18 | 0 | 7 | 22.6% | 38.9% |
| 40202 | 77 | 16 | 53 | 0 | 16 | 20.08% | 30.2% |
| 40203 | 41 | 9 | 17 | 0 | 9 | 22.0% | 52.9% |
| 40210 | 24 | 5 | 16 | 0 | 5 | 20.8% | 31.3% |
| 40321 | 39 | 8 | 12 | 0 | 8 | 20.5% | 66.7% |
| 40324 | 69 | 14 | 30 | 0 | 14 | 20.3% | 46.7% |
| 40421 | 97 | 20 | 11 | 9 | 11 | 11.3% | 100.0% |
| 40424 | 84 | 17 | 18 | 0 | 17 | 20.2% | 94.4% |
| 43800 | 38 | 8 | 3 | 5 | 3 | 7.9% | 100.0% |
| 43920 | 35 | 7 | 2 | 5 | 2 | 5.7% | 100.0% |
| 48800 | 33 | 7 | 15 | 0 | 7 | 21.2% | 46.7% |
| 49810 | 61 | 13 | 32 | 0 | 13 | 21.3% | 40.6% |
| Stratum:
1st digit – Region: (1) Northeast, (2) Midwest, (3) South, (4) West 2nd digit – Trauma: (0) Not a trauma center, (1) Trauma center level I, (2) Trauma center level II, (3) Trauma center level III, Collapsed categories used for strata with small sample sizes: (8) Trauma center level I or II, (9) Trauma center level I, II, or III 3rd digit – Urban-rural location: (1) Large metropolitan, (2) Small metropolitan, (3) Micropolitan, (4) Non-urban residual, Collapsed categories used for strata with small sample sizes: (8) Metropolitan (large and small), (9) Non-metropolitan (micropolitan and non-urban location) 4th digit – Teaching: (0) Metropolitan non-teaching, (1) Metropolitan teaching, (2) Non-metropolitan teaching and non-teaching 5th digit – Control: (0) All (used for combining public, voluntary, and private), (1) Public - government, non-Federal, (2) Voluntary - private, non-profit, (3) Proprietary – private, investor-owned/for-profit, (4) Private (used for combining private voluntary and proprietary) | |||||||
Appendix II: State-Specific Restrictions
The table below enumerates the types of restrictions applied to the 2007 Nationwide Emergency Department Sample. Restrictions include the following types:
For each restriction type the data sources are listed alphabetically by State. Only data sources that have restrictions are included. Data sources that do not have restrictions are not included.
Table 1. State-Specific Restrictions
| Confidentiality of Hospitals |
|---|
Limitations on sampling are required to ensure hospital confidentiality:
|
| Confidentiality of Records |
Limitations on selected data elements are required by the following data sources to ensure patient confidentiality:
|
| Limited Reporting of External Cause of Injury Codes |
The following data sources have limitations on the reporting of external cause of injury codes (E codes):
|
| Missing Discharges for Specific Populations of Patients |
The following data sources may be missing discharge records for specific populations of patients:
|
| Type of Data Element |
HCUP Data Element |
Coding Notes |
|---|---|---|
| Admission timing | AWEEKEND | Admission on weekend: (0) admission on Monday-Friday, (1) admission on Saturday-Sunday |
| AMONTH | Admission month coded from (1) January to (12) December | |
| Age at admission | AGE | Age in years coded 0-124 years |
| Diagnosis information | DX1 – DX15 | ICD-9-CM diagnoses |
| DXCCS1 – DXCCS15 | Clinical Classifications Software (CCS) category for all diagnoses | |
| CHRON1 – CHRON15 | Chronic condition indicator for all diagnoses: (0) non-chronic condition, (1) chronic condition | |
| NDX | Number of diagnoses coded on the original record. A maximum of 15 codes are retained on the NEDS. | |
| INTENT_SELF_HARM | Diagnosis reported on records indicates intended self harm: (0) not intended self harm, (1) intended self harm | |
| Discharge timing | DQTR | Coded: (1) Jan - Mar, (2) Apr - Jun, (3) Jul - Sep, (4) Oct - Dec |
| YEAR | Calendar year of ED visits | |
| Disposition of patient from the ED | DISP_ED | Disposition from ED: (1) routine, (2) transfer to short-term hospital, (5) other transfers, including skilled nursing facility, intermediate care, and another type of facility, (6) home healthcare, (7) against medical advice, (9) admitted as an inpatient to this hospital, (20) died in ED, (98) not admitted, destination unknown, (99) discharged alive, destination unknown (but not admitted) |
| DIED_VISIT | Died in ED: (0) did not die (1) died in the ED, (2) died in the hospital | |
| ED event | EDevent | Type of ED event: (1) ED visit in which the patient is treated and released, (2) ED visit in which the patient is admitted to this same hospital, (3) ED visit in which the patient is transferred to another short-term hospital, (9) ED visit in which the patient died in the ED, (98) ED visits in which patient was not admitted, destination unknown, (99) ED visit in which patient was discharged alive, destination unknown (but not admitted) |
| External causes of injury and poisoning | ECODE1 – ECODE4 | External cause of injury and poisoning codes (ICD-9-CM). |
| E_CCS1 – E_CCS4 | CCS category for the external cause of injury and poisoning codes | |
| NECODE | Number of external cause of injury codes on the original record. A maximum of 4 codes are retained on the NEDS. | |
| Sex of patient | FEMALE | Indicates sex: (0) male, (1) female |
| Urban-rural location of the patient’s residence | PL_NHCS2006 | Urban–rural designation for patient’s county of residence: (1) large central metropolitan, (2) large fringe metropolitan, (3) medium metropolitan, (4) small metropolitan, (5) micropolitan, (6) not metropolitan or micropolitan |
| National quartile for median household income of patient's ZIP Code | ZIPINC_QRTL | Median household income quartiles for patient's ZIP Code. For 2007, the median income quartiles are defined as: (1) $1 - $38,999; (2) $39,000 - $47,999; (3) $48,000 - $60,999; and (4) $63,000 or more. |
| Payer information | PAY1 | Expected primary payer, uniform: (1) Medicare, (2) Medicaid, (3) private including HMO, (4) self-pay, (5) no charge, (6) other |
| PAY2 | Expected secondary payer, uniform: (1) Medicare, (2) Medicaid, (3) private including HMO, (4) self-pay, (5) no charge, (6) other | |
| Total ED charges | TOTCHG_ED | Total charges for ED services, edited |
| HCUP source file | HCUPFILE | Source of HCUP record: (SEDD) from SEDD file, (SID) from SID file |
| Discharge weight | DISCWT | Discharge weight used to calculate national estimates. Weights ED visits to AHA universe. |
| Hospital identifier, synthetic | HOSP_ED | Unique HCUP NEDS hospital number – links to NEDS Hospital Weights file, but not to other HCUP databases |
| Hospital information | HOSP_REGION | Region of hospital: (1) Northeast, (2) Midwest, (3) South, (4) West |
| NEDS_STRATUM | Stratum used to sample hospitals, based on geographic region, trauma, location/teaching status, and control. Stratum information is also contained in the Hospital Weights file. | |
| Record identifier, synthetic | KEY_ED | Unique HCUP NEDS record number – links to NEDS Supplemental files, but not to other HCUP databases |
| Type of Data Element |
HCUP Data Element |
Coding Notes |
|---|---|---|
| CPT procedure information | CPT1 – CPT15 | CPT/HCPCS procedures performed in the ED |
| NCPT | Number of procedures coded on the original record. A maximum of 15 CPT codes are retained on the NEDS. | |
| ICD-9-CM procedure information | PR_ED1 – PR_ED9 | ICD-9-CM procedures performed in ED |
| PRCCS_ED1 – PRCCS_ED9 | Clinical Classifications Software (CCS) category for all ICD-9-CM procedures | |
| PCLASS_ED1 – PCLASS_ED9 | Procedure class for all ICD-9-CM procedures: (1) Minor Diagnostic, (2) Minor Therapeutic, (3) Major Diagnostic, (4) Major Therapeutic | |
| NPR_ED | Number of procedures coded on the original record. A maximum of 9 ICD-9-CM procedure codes are retained on the NEDS. | |
| HCUP source file | HCUPFILE | Source of HCUP record: (SEDD) from SEDD file, (SID) from SID file |
| Discharge weight | DISCWT | Discharge weight used to calculate national estimates. Weights ED visits to AHA universe. |
| Hospital identifier, synthetic | HOSP_ED | Unique HCUP NEDS hospital number – links to NEDS Hospital Weights file, but not to other HCUP databases |
| Record identifier, synthetic | KEY_ED | Unique HCUP NEDS record number – links to NEDS Supplemental files, but not to other HCUP databases |
| Type of Data Element |
HCUP Data Element |
Coding Notes |
|---|---|---|
| Disposition of patient from the hospital | DISP_IP | Disposition from hospital admission: (1) routine, (2) transfer to short-term hospital, (5) other transfers, including skilled nursing facility, intermediate care, and another type of facility, (6) home healthcare, (7) against medical advice, (20) died in hospital, (99) discharged alive, destination unknown |
| Diagnosis Related Group (DRG) | DRG | DRG in use on discharge date |
| DRGVER | Grouper version in use on discharge date | |
| MDC | Major Diagnosis Category (MDC) in use on discharge date | |
| Length of hospital inpatient stay | LOS_IP | Length of stay, edited |
| Total charges for inpatient stay | TOTCHG_IP | Total charges for ED and inpatient services, edited |
| ICD-9-CM procedure information | PR_IP1 – PR_IP9 | ICD-9-CM procedures coded on ED admissions. Procedure may have been performed in the ED or during the hospital stay. |
| PRCCS_IP1 – PRCCS_IP9 | Clinical Classifications Software (CCS) category for all ICD-9-CM procedures | |
| PCLASS_IP1 – PCLASS_IP9 | Procedure class for all ICD-9-CM procedures: (1) Minor Diagnostic, (2) Minor Therapeutic, (3) Major Diagnostic, (4) Major Therapeutic | |
| NPR_IP | Number of procedures coded on the original record. A maximum of 9 ICD-9-CM procedure codes are retained on the NEDS. | |
| HCUP source file | HCUPFILE | Source of HCUP record: (SEDD) from SEDD file, (SID) from SID file |
| Discharge weight | DISCWT | Discharge weight used to calculate national estimates. Weights ED visits to AHA universe. |
| Hospital identifier, synthetic | HOSP_ED | Unique HCUP NEDS hospital number – links to NEDS Hospital Weights file, but not to other HCUP databases |
| Record identifier, synthetic | KEY_ED | Unique HCUP NEDS record number – links to NEDS Supplemental files, but not to other HCUP databases |
| Type of Data Element |
HCUP Data Element |
Coding Notes |
|---|---|---|
| Discharge counts | N_DISC_U | Number of AHA universe ED visits in the stratum |
| S_DISC_U | Number of sampled ED visits in the sampling stratum | |
| TOTAL_EDvisits | Total number of ED visits for this hospital in the NEDS | |
| Discharge weights | DISCWT | Discharge weight used to calculate national estimates. Weights ED visits to AHA universe. |
| Discharge Year | YEAR | Discharge year |
| Hospital counts | N_HOSP_U | Number of AHA universe hospital-based EDs in the stratum |
| S_HOSP_U | Number of sampled hospital-based EDs in the stratum | |
| Hospital identifier, synthetic | HOSP_ED | Unique HCUP NEDS hospital number – links to NEDS Hospital Weights file, but not to other HCUP databases |
| Hospital characteristics | HOSP_URCAT4 | Hospital urban-rural location: (1) large metropolitan areas with at least 1 million residents, (2) small metropolitan areas with less than 1 million residents, (3) micropolitan areas, (4) not metropolitan or micropolitan, (8) metropolitan, collapsed category of large and small metropolitan, (9) non-metropolitan, collapsed category of micropolitan and rural |
| HOSP_CONTROL | Control/ownership of hospital: (0) government or private, collapsed category, (1) government, nonfederal, public, (2) private, non-profit, voluntary, (3) private, invest-own, (4) private, collapsed category | |
| HOSP_REGION | Region of hospital: (1) Northeast, (2) Midwest, (3) South, (4) West | |
| HOSP_TRAUMA | Trauma center level: (0) non-trauma center, (1) trauma level I, (2) trauma level II (3) trauma level III, (8) trauma level I or II, collapsed category (9) trauma level I, II, or III, collapsed category | |
| HOSP_UR_TEACH | Teaching status of hospital: (0) metropolitan non-teaching, (1) metropolitan teaching, (2) non-metropolitan | |
| NEDS_STRATUM | Stratum used to sample EDs, includes geographic region, trauma, location/teaching status, and control | |
| Hospital weight | HOSPWT | Weight to hospital-based EDs in AHA universe (i.e., total U.S.) |
Appendix IV: Comparisons of the NEDS with Existing Sources of ED Data
Figure 1. Emergency Department Visit Counts (in thousands) in the United States, 2007
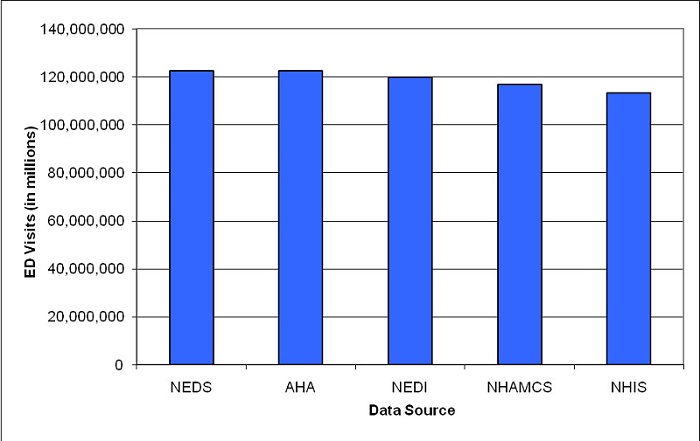
Notes: ED = emergency department; NEDS = HCUP Nationwide Emergency Department Sample; AHA = American Hospital Association Annual Survey Database; NEDI=National Emergency Department Inventory – USA; NHAMCS = National Hospital Ambulatory Medical Care Survey; NHIS = National Health Interview Survey.
Table 1. Estimates of ED Visits by U.S. Geographic Region from Five ED Data Sources, 2007
| ED Visits | ED Data Source | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NEDS1 | AHA | NEDI | NHAMCS | NHIS 2 | ||||||
| N (weighted) | % | N | % | N | % | N (weighted) | % | N (weighted) | % | |
| By Census Region | ||||||||||
| Northeast | 23,988,430 | 20% | 23,988,430 | 20% | 22,413,606 | 19% | 20,484,250 | 18% | 20,558,722 | 18% |
| Midwest | 28,708,265 | 23% | 28,708,265 | 23% | 27,518,173 | 23% | 25,062,048 | 21% | 26,832,753 | 24% |
| South | 48,039,208 | 39% | 48,039,208 | 39% | 48,506,546 | 41% | 48,712,961 | 42% | 43,229,235 | 38% |
| West | 21,595,836 | 18% | 21,595,836 | 18% | 21,240,507 | 18% | 22,542,807 | 19% | 22,472,536 | 20% |
| Total U.S. | 122,331,739 | 100% | 122,331,739 | 100% | 119,678,832 | 100% | 116,802,066 | 100% | 113,093,245 | 100% |
| Notes: ED = emergency department; NEDS = HCUP Nationwide Emergency Department Sample; AHA = American Hospital Association Annual Survey Database; NEDI = National Emergency Department Inventory - USA; NHAMCS = National Hospital Ambulatory Medical Care Survey; NHIS = National Health Interview Survey.
1 NEDS weighted counts by geographic region exactly match the AHA counts because the AHA data were used as control totals for the NEDS discharge weights. 2 NHIS estimates were calculated using the midpoint of the ranges provided in the survey (0, 1, 2-3, 4-5, 6-7, 8-9, 10-12, and 13-15). For the upper range of visits in the survey (16 or more ED visits), 16 ED visits were used for the estimate. |
||||||||||
Table 2. Estimates of the ED Visits Resulting in Inpatient Admissions (Admission Rate) by U.S. Geographic Region from Two ED Data Sources, 2007
| ED Visits Resulting in Inpatient Admissions | ED Data Sources | |||
|---|---|---|---|---|
| NEDS | NHAMCS | |||
| N (weighted) | % of all ED Visits | N (weighted) | % of all ED Visits | |
| By Census Region | ||||
| Northeast | 4,322,702 | 18% | 2,926,341 | 14% |
| Midwest | 4,070,450 | 14% | 3,616,329 | 14% |
| South | 7,448,211 | 16% | 5,376,689 | 11% |
| West | 3,225,115 | 15% | 2,719,653 | 12% |
| Total U.S. | 19,066,478 | 16% | 14,639,012 | 13% |
| Notes: ED = emergency department; NEDS = HCUP Nationwide Emergency Department Sample; NHAMCS = National Hospital Ambulatory Medical Care Survey. | ||||
Table 3. Estimates of the Number of Hospital-Based EDs by ED Visit Volume from Three ED Data Sources, 2007
| Volume of ED Visits in 2007 | Data Sources | |||||
|---|---|---|---|---|---|---|
| NEDS | AHA | NEDI | ||||
| N (weighted) | % | N (weighted) | % | N (weighted) | % | |
| Less than 10,000 visits | 1,313 | 27% | 1,692 | 35% | 1,503 | 31% |
| 10,000 - 19,999 visits | 957 | 20% | 898 | 19% | 1,032 | 21% |
| 20,000 - 29,999 visits | 776 | 16% | 664 | 14% | 731 | 15% |
| 30,000 - 39,999 visits | 620 | 13% | 495 | 10% | 621 | 13% |
| 40,000 - 49,999 visits | 370 | 8% | 359 | 7% | 396 | 8% |
| 50,000 or more visits | 773 | 16% | 701 | 15% | 591 | 12% |
| All Hospital-based EDs | 4,809 | 100% | 4,809 | 100% | 4,874 | 100% |
| Notes: ED = emergency department; NEDS = Nationwide Emergency Department Sample from the Healthcare Cost and Utilization Project; AHA = American Hospital Association Annual Survey Database; NEDI = National Emergency Department Inventory - USA. | ||||||
Table 4. Estimates of the Number of Injury-Related ED Visits from Three ED Data Sources, 2007
| Data Sources | |||
|---|---|---|---|
| NEDS1 | NHAMCS1 | NEISS-AIP3 | |
| Total number of ED visits for injuries (weighted) | 27,615,496 | 27,946,076 | 29,756,586 |
| Notes: ED = emergency department; NEDS = Nationwide Emergency Department Sample from the Healthcare Cost and Utilization Project; NHAMCS = National Hospital Ambulatory Medical Care Survey; NEISS-AIP = National Electronic Injury Surveillance System All-Injury Program.
1 Any non-fatal ED visit with an injury diagnosis of 800-909.2, 909.4, 090.9, 910-994.9, 995.5-995.59, 995.80-995.85. For the NEDS, injuries were identified using the principal diagnosis (DX1) for ED admissions and all diagnoses otherwise. 2 Data from WISQARS Query System (http://webappa.cdc.gov/sasweb/ncipc/nfirates.html). Includes non-fatal, all-cause injuries. Patients who died on arrival to the ED or during treatment in the ED are excluded. Queried November 13, 2009. |
|||
1 Merrill and Owens, 2007
2 Merrill and Owens, 2007
3 MacKenzie EJ, Hoyt DB, Sacra JC, et al. National inventory of hospital trauma centers. JAMA. 2003;289:1515-1522.
4 American Trauma Society. Trauma Information Exchange Program. Available at: http://www.amtrauma.org/?page=TIEP. ![]() Accessed April 2005.
Accessed April 2005.
5 United States Department of Agriculture Economic Research Service, 2007
6 Carlson BL, Johnson AE, Cohen SB. "An Evaluation of the Use of Personal Computers for Variance Estimation with Complex Survey Data." Journal of Official Statistics, vol. 9, no. 4, 1993: 795-814.