STATISTICAL BRIEF #247 |
January 2019
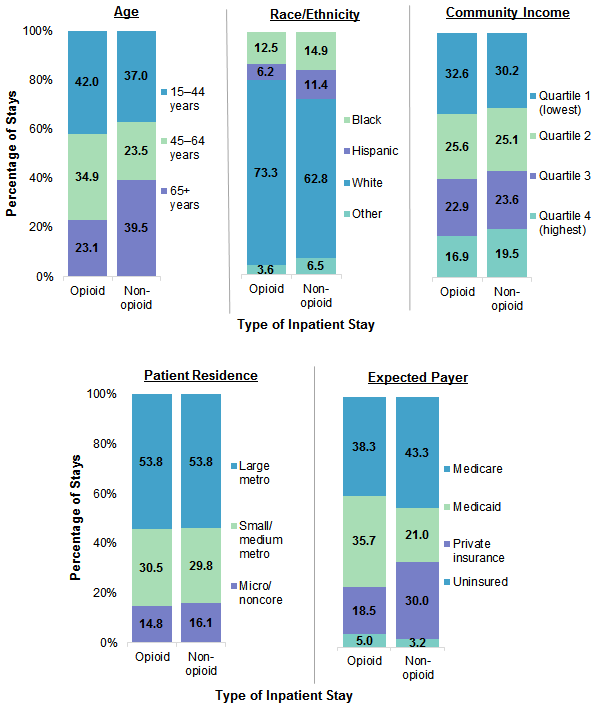
Audrey J. Weiss, Ph.D., Kimberly W. McDermott, Ph.D., and Kevin C. Heslin, Ph.D. Introduction The opioid epidemic is a national crisis, but research suggests that some subgroups of the population, such as women, may be more affected than other groups. For example, compared with men, women are more likely to be prescribed painkillers and are likely to be prescribed them in higher doses and to become dependent on them more quickly.1,2 The rate of opioid-related hospitalizations3 and deaths4 has been increasing faster in recent years among women than men. Indeed, in most states in 2014, women had higher opioid-related hospitalization rates than men.5 Among women, some subgroups may be more severely affected by the opioid crisis than others. Substantial differences in opioid use exist based on characteristics of women such as age, race/ethnicity, income, payer, and geography. For example, compared with Black and Hispanic women, White women are more likely to have long-term use of prescription opioids and are likely to have higher rates of drug overdose deaths involving prescription or illegal opioids.6,7 Women aged 65 years and older have a higher prevalence of long-term prescription opioid use for noncancer pain than do women under age 65 years.8 Even within age groups, differences may exist. For instance, among women of reproductive age (15-44 years), prescription opioid use is higher among those with Medicaid than among those with private insurance.9 This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents statistics on opioid-related hospitalizations among women aged 15 years and older using the 2016 National Inpatient Sample (NIS). The distribution of opioid-related stays by select patient and hospitalization characteristics is presented and contrasted with the distribution for non-opioid-related stays. The types of opioid diagnoses during hospitalization are also provided for select patient characteristics. Finally, rates of opioid-related stays are presented by patient characteristics. Differences greater than 10 percent between estimates are noted in the text. Findings Distribution of opioid-related inpatient stays among women by patient characteristics, 2016 Figure 1 presents characteristics of opioid-related versus nonopioid-related stays among women in 2016. |
|
|
Figure 1. Characteristics of opioid-related versus non-opioid-related inpatient stays among women, 2016
Abbreviations: Metro, metropolitan; micro, micropolitan Bar chart that shows percentage of age, race/ethnicity, community income, patient residence, and expected payer characteristics of opioid-related and non-opioid-related inpatient stays among women in 2016. Data are provided in Supplemental Table 1.
|
|
|
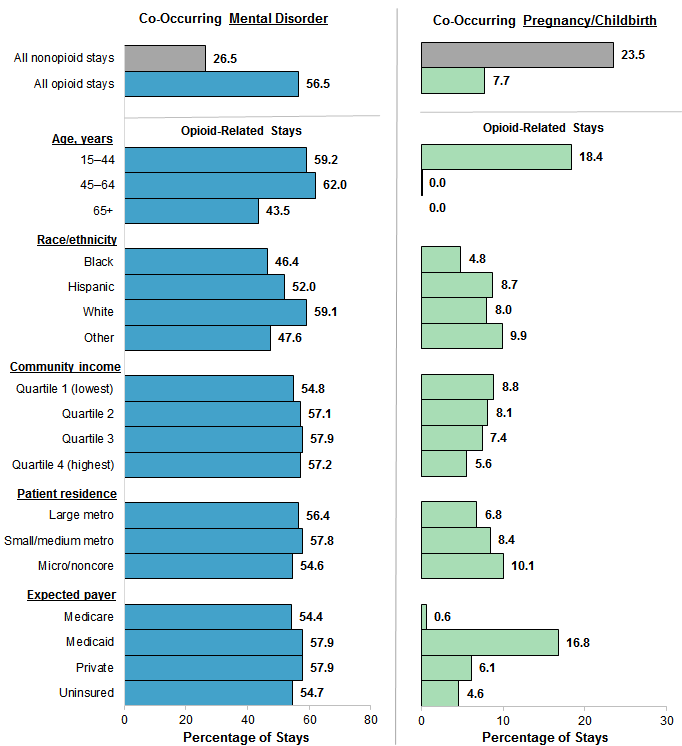
Figure 2. Co-occurring mental disorder or pregnancy/childbirth for opioid-related inpatient stays among women, by patient characteristics, 2016
Abbreviations: Metro, metropolitan; micro, micropolitan Bar chart that shows opioid-related inpatient stays among women with a co-occurring mental health diagnosis or pregnancy/childbirth by patient characteristics in 2016. Data are provided in Supplemental Table 2. |
|
|
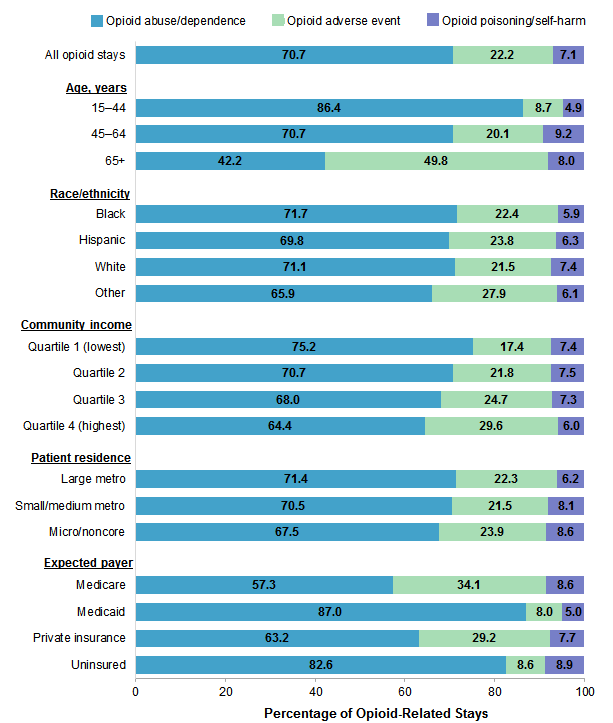
Figure 3. Type of opioid diagnosis for opioid-related inpatient stays among women, by patient characteristics, 2016
Abbreviations: Metro, metropolitan; micro, micropolitan Bar chart that shows the percentage of opioid-related inpatient stays among women for opioid abuse-dependence, opioid adverse event, and opioid poisoning/self-harm in 2016. Data are provided in Supplemental Table 3. |
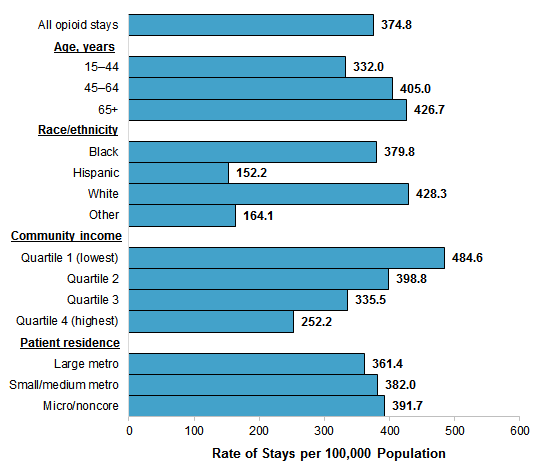
Figure 4 presents the rate per 100,000 population of opioid-related stays among women overall and by age, race/ethnicity, community-level income, and patient residence in 2016. |
|
Figure 4. Population rate of opioid-related inpatient stays among women overall and by patient characteristics, 2016
Abbreviations: Metro, metropolitan; micro, micropolitan Bar chart that shows the rate of opioid-related inpatient stays among women per 100,000 population by patient characteristics in 2016. Data are provided in Supplemental Table 4.
|
|
|
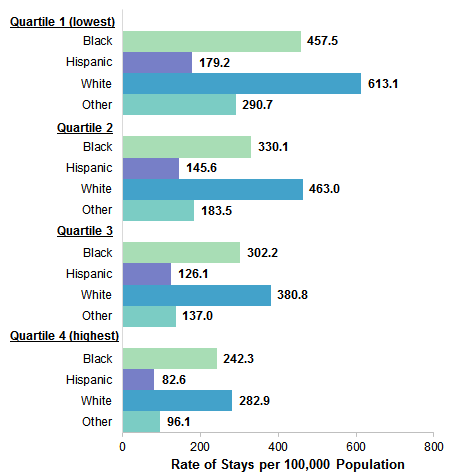
Figure 5. Population rate of opioid-related inpatient stays among women by community-level income quartile and race/ethnicity, 2016
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2016 Bar chart that shows the rate of opioid-related inpatient stays per 100,000 population among women by community-level income quartile and race/ethnicity in 2016. Data are provided in Supplemental Table 5. |
|
|
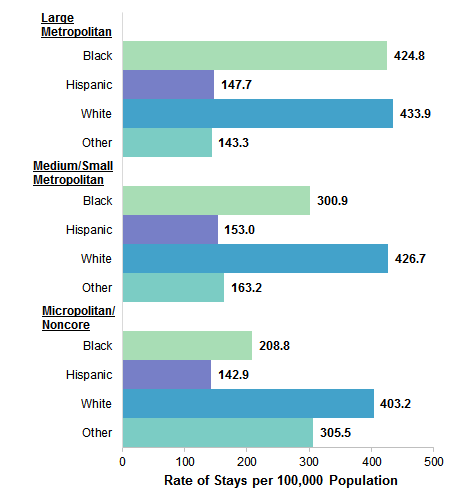
Figure 6. Population rate of opioid-related inpatient stays among women by patient residence and race/ethnicity, 2016
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2016 Bar chart that shows the rate of opioid-related inpatient stays per 100,000 population among women by patient residence and race/ethnicity in 2016. Data are provided in Supplemental Table 5. |
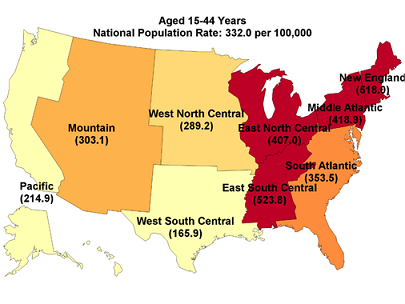
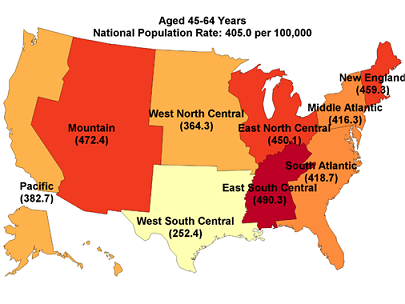
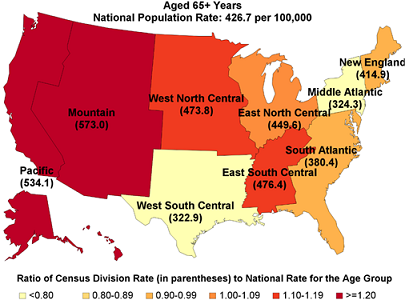
Figure 7 provides the population rate of opioid-related inpatient stays among women aged 15-44 years, 45-64 years, and 65 years and older by U.S. census division in 2016. The ratio of each census division rate to the national rate also is provided in the figure and is reflected in the color-coding of the maps. |
|
Figure 7. Population rate of opioid-related inpatient stays among women by age group and census division, and ratio of census division to national rate, 2016 |
|
|
|
About Statistical Briefs
Healthcare Cost and Utilization Project (HCUP) Statistical Briefs provide basic descriptive statistics on a variety of topics using HCUP administrative healthcare data. Topics include hospital inpatient, ambulatory surgery, and emergency department use and costs, quality of care, access to care, medical conditions, procedures, and patient populations, among other topics. The reports are intended to generate hypotheses that can be further explored in other research; the reports are not designed to answer in-depth research questions using multivariate methods. Data Source The estimates in this Statistical Brief are based upon data from the HCUP 2016 National Inpatient Sample (NIS). Supplemental sources included population denominator data for use with HCUP databases, derived from information available from Claritas, a vendor that compiles and adds value to data from the U.S. Census Bureau.10 Definitions Diagnoses, ICD-10-CM/PCS, and major diagnostic categories (MDCs) The principal diagnosis is that condition established after study to be chiefly responsible for the patient's admission to the hospital. Secondary diagnoses are concomitant conditions that coexist at the time of admission or develop during the stay. All-listed diagnoses include the principal diagnosis plus these additional secondary conditions. ICD-10-CM/PCS is the International Classification of Diseases, Tenth Revision, Clinical Modification/Procedure Coding System. In October 2015, ICD-10-CM/PCS replaced the ICD-9-CM diagnosis coding system with the ICD-10-CM diagnosis coding system for most inpatient and outpatient medical encounters. There are over 70,000 ICD-10-CM diagnosis codes. MDCs assign ICD-10-CM principal diagnosis codes to 1 of 25 general diagnosis categories. Case definition Opioid-related hospital use was identified using the all-listed ICD-10-CM diagnosis codes shown in Table 1. |
| Table 1. ICD-10-CM diagnosis codes defining different opioid-related conditions | ||
| Type of opioid-related condition | ICD-10-CM diagnosis codes | |
|---|---|---|
| Abuse or dependence | F11 series: Opioid-related disorders (except F11.21) | |
| Adverse event | T40.0X5: Adverse effect of opium T40.2X5: Adverse effect of other opioids T40.3X5: Adverse effect of methadone T40.4X5: Adverse effect of other synthetic narcotics T40.605: Adverse effect of unspecified narcotics T40.695: Adverse effect of other narcotics |
|
| Poisoning, including self-harm | T40.0X1, 0X2, 0X3, 0X4: Poisoning by opium-accidental, intentional self-harm, assault, or undetermined T40.1X1, 1X2, 1X3, 1X4: Poisoning by heroin-accidental, intentional self-harm, assault, or undetermined T40.2X1, 2X2, 2X3, 2X4: Poisoning by other opioids-accidental, intentional self-harm, assault, or undetermined T40.3X1, 3X2, 3X3, 3X4: Poisoning by methadone-accidental, intentional self-harm, assault, or undetermined T40.4X1, 4X2, 4X3, 4X4: Poisoning by other synthetic narcotics-accidental, intentional self-harm, assault, or undetermined T40.601-T40.604: Poisoning by unspecified narcotics-accidental, intentional self-harm, assault, or undetermined T40.691-T40.694: Poisoning by other narcotics-accidental, intentional self-harm, assault, or undetermined |
|
| Abbreviation: ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification | ||
Co-occurring mental disorders were defined using the ICD-10-CM codes provided in the separate appendix associated with this Statistical Brief on the HCUP-US website at www.hcup-us.ahrq.gov/reports/statbriefs/sb247-appendix.pdf. Co-occurring pregnancy/childbirth was defined as MDC 14 (pregnancy, childbirth and puerperium).
Types of hospitals included in the HCUP National Inpatient Sample The National Inpatient Sample (NIS) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NIS includes obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Beginning in 2012, long-term acute care hospitals are also excluded. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay will be included in the NIS. Unit of analysis The unit of analysis is the hospital discharge (i.e., the hospital stay), not a person or patient. This means that a person who is admitted to the hospital multiple times in 1 year will be counted each time as a separate discharge from the hospital. Location of patients' residence Place of residence is based on the urban-rural classification scheme for U.S. counties developed by the National Center for Health Statistics (NCHS) and based on the Office of Management and Budget (OMB) definition of a metropolitan service area as including a city and a population of at least 50,000 residents:
Community-level income is based on the median household income of the patient's ZIP Code of residence. Quartiles are defined so that the total U.S. population is evenly distributed. Cut-offs for the quartiles are determined annually using ZIP Code demographic data obtained from Claritas, a vendor that adds value to data from the U.S. Census Bureau.11 The value ranges for the income quartiles vary by year. The income quartile is missing for patients who are homeless or foreign. Payer Payer is the expected payer for the hospital stay. To make coding uniform across all HCUP data sources, payer combines detailed categories into general groups:
For this Statistical Brief, when more than one payer is listed for a hospital discharge, the first-listed payer is used. Division Division corresponds to the location of the hospital and is one of the nine divisions defined by the U.S. Census Bureau:
Data on Hispanic ethnicity are collected differently among the States and also can differ from the census methodology of collecting information on race (White, Black, Asian/Pacific Islander, American Indian/Alaska Native, Other [including mixed race]) separately from ethnicity (Hispanic, non-Hispanic). State data organizations often collect Hispanic ethnicity as one of several categories that include race. Therefore, for multistate analyses, HCUP creates the combined categorization of race and ethnicity for data from States that report ethnicity separately. When a State data organization collects Hispanic ethnicity separately from race, HCUP uses Hispanic ethnicity to override any other race category to create a Hispanic category for the uniformly coded race/ethnicity data element, while also retaining the original race and ethnicity data. This Statistical Brief reports race/ethnicity for the following categories: Hispanic, non-Hispanic White, non-Hispanic Black, and other race/ethnic groups (which includes Asian/Pacific Islander, American Indian/Alaska Native, and non-Hispanic Other). About HCUP The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska Department of Health and Social Services Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association Delaware Division of Public Health District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi State Department of Health Missouri Hospital Industry Data Institute Montana Hospital Association Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Department of Health and Human Resources, West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About the NIS The HCUP National (Nationwide) Inpatient Sample (NIS) is a nationwide database of hospital inpatient stays. The NIS is nationally representative of all community hospitals (i.e., short-term, non-Federal, nonrehabilitation hospitals). The NIS includes all payers. It is drawn from a sampling frame that contains hospitals comprising more than 95 percent of all discharges in the United States. The vast size of the NIS allows the study of topics at the national and regional levels for specific subgroups of patients. In addition, NIS data are standardized across years to facilitate ease of use. Over time, the sampling frame for the NIS has changed; thus, the number of States contributing to the NIS varies from year to year. The NIS is intended for national estimates only; no State-level estimates can be produced. The unweighted sample size for the 2016 NIS is 7,135,090 (weighted, this represents 35,675,421 inpatient stays). For More Information For other information on mental and substance abuse disorders, refer to the HCUP Statistical Briefs located at www.hcup-us.ahrq.gov/reports/statbriefs/sb_mhsa.jsp. For additional HCUP statistics, visit:
For a detailed description of HCUP and more information on the design of the National Inpatient Sample (NIS) please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the National (Nationwide) Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated February 2018. www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed February 12, 2018. Suggested Citation Weiss AJ (IBM Watson Health), McDermott KW (IBM Watson Health), Heslin KC (AHRQ). Opioid-Related Hospital Stays Among Women, 2016. HCUP Statistical Brief #247. January 2019. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb247-Opioid-Hospital-Stays-Women.pdf. Acknowledgments The authors would like to acknowledge the contributions of Minya Sheng of IBM Watson Health. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:Joel W. Cohen, Ph.D., Director Center for Financing, Access and Cost Trends Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 This Statistical Brief was posted online on January 22, 2019. 1 Centers for Disease Control and Prevention. Prescription Painkiller Overdoses: A Growing Epidemic, Especially Among Women. Updated September 4, 2018. https://www.cdc.gov/vitalsigns/prescriptionpainkilleroverdoses/index.html. Accessed December 10, 2018. 2 U.S. Food and Drug Administration. Women and Pain Medicines. Updated October 1, 2018. https://www.fda.gov/ForConsumers/ByAudience/ForWomen/WomensHealthTopics/ucm621707.htm. Accessed December 10, 2018. 3 Weiss AJ, Bailey MK, O'Malley L, Barret ML, Elixhauser A, Steiner CA. Patient Characteristics and Opioid-Related Inpatient Stays and Emergency Department Visits Nationally and by State, 2014. HCUP Statistical Brief #224. June 2017. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb224-Patient-Characteristics-Opioid-Hospital-Stays-ED-Visits-by-State.pdf. Accessed September 26, 2018. 4 Mack KA, Jones CM, Paulozzi LJ. Vital signs: overdoses of prescription opioid pain relievers and other drugs among women—United States, 1999-2010. Morbidity and Mortality Weekly Report. 2013;62(26):537-42. 5 Weiss et al., 2017. Op.cit. 6 Frenk SM, Porter KS, Paulozzi LJ. Prescription Opioid Analgesic Use Among Adults: United States, 1999-2012. NCHS Data Brief #189. February 2015. Centers for Disease Control and Prevention. www.cdc.gov/nchs/data/dataBriefs/db189.pdf. Accessed September 26, 2018. 7 Seth P, Scholl L, Rudd RA, Bacon S. Overdose deaths involving opioids, cocaine, and psychostimulants—United States, 2015-2016. Morbidity and Mortality Weekly Report. 2018;67(12):349-58. 8 Campbell CI, Weisner C, LeResche L, Ray T, Saunders K, Sullivan MD, et al. Age and sex trends in long-term opioid analgesic use for noncancer pain. American Journal of Public Health. 2010;100(12):2541-7. 9 Ailes EC, Dawon AL, Lind JN, Gilboa SM, Frey MT, Broussard CS, et al. Opioid prescription claims among women of reproductive age—United States, 2008-2012. Morbidity and Mortality Weekly Report. 2015;64(2):37-41. 10 Claritas. Claritas Demographic Profile by ZIP Code. https://claritas360.claritas.com/mybestsegments/. |
| Supplemental Table 1. Characteristics of opioid-related versus nonopioid-related inpatient stays among women in 2016 for data presented in Figure 1 | ||
| Characteristic | Opioid stays, % | Non-opioid-related stays, % |
|---|---|---|
| Age, years | ||
| 15-44 | 42.0 | 37.0 |
| 45-64 | 34.9 | 23.5 |
| 65+ | 23.1 | 39.5 |
| Race/ethnicity | ||
| Black | 12.5 | 14.9 |
| Hispanic | 6.2 | 11.4 |
| White | 73.3 | 62.8 |
| Other | 3.6 | 6.5 |
| Community income | ||
| Quartile 1 (lowest) | 32.6 | 30.2 |
| Quartile 2 | 25.6 | 25.1 |
| Quartile 3 | 22.9 | 23.6 |
| Quartile 4 (highest) | 16.9 | 19.5 |
| Patient residence | ||
| Large metropolitan | 53.8 | 53.8 |
| Small/medium metropolitan | 30.5 | 29.8 |
| Micropolitan/noncore | 14.8 | 16.1 |
| Expected payer | ||
| Medicare | 38.3 | 43.3 |
| Medicaid | 35.7 | 21.0 |
| Private insurance | 18.5 | 30.0 |
| Uninsured | 5.0 | 3.2 |
| Supplemental Table 2. Co-occurring mental health diagnosis or pregnancy/childbirth for opioid-related inpatient stays among women, by patient characteristics in 2016 for data presented in Figure 2 | ||
| Characteristic | Stays with a co-occurring mental health diagnosis, % | Stays with a co-occurring pregnancy/childbirth, % |
|---|---|---|
| All nonopioid stays | 26.5 | 23.5 |
| All opioid stays | 56.5 | 7.7 |
| Age, years | ||
| 15-44 | 59.2 | 18.4 |
| 45-64 | 62.0 | 0.0 |
| 65+ | 43.5 | 0.0 |
| Race/ethnicity | ||
| Black | 46.4 | 4.8 |
| Hispanic | 52.0 | 8.7 |
| White | 59.1 | 8.0 |
| Other | 47.6 | 9.9 |
| Community income | ||
| Quartile 1 (lowest) | 54.8 | 8.8 |
| Quartile 2 | 57.1 | 8.1 |
| Quartile 3 | 57.9 | 7.4 |
| Quartile 4 (highest) | 57.2 | 5.6 |
| Patient residence | ||
| Large metropolitan | 56.4 | 6.8 |
| Small/medium metropolitan | 57.8 | 9.0 |
| Micropolitan/noncore | 54.6 | 10.1 |
| Expected payer | ||
| Medicare | 54.4 | 0.6 |
| Medicaid | 57.9 | 16.8 |
| Private insurance | 57.9 | 6.1 |
| Uninsured | 54.7 | 4.6 |
| Supplemental Table 3. Type of opioid diagnosis for opioid-related inpatient stays among women, by patient characteristics in 2016 for data presented in Figure 3 | |||
| Characteristic | Stays for opioid abuse dependence, % | Stays for opioid adverse event, % | Stays for opioid poisoning/self-harm, % |
|---|---|---|---|
| All opioid stays | 70.7 | 22.2 | 7.1 |
| Age, years | |||
| 15-44 | 86.4 | 8.7 | 4.9 |
| 45-64 | 70.7 | 20.1 | 9.2 |
| 65+ | 42.2 | 49.8 | 8.0 |
| Race/ethnicity | |||
| Black | 71.7 | 22.4 | 5.9 |
| Hispanic | 69.8 | 23.8 | 6.3 |
| White | 71.1 | 21.5 | 7.4 |
| Other | 65.9 | 27.9 | 6.1 |
| Community income | |||
| Quartile 1 (lowest) | 75.2 | 17.4 | 7.4 |
| Quartile 2 | 70.7 | 21.8 | 7.5 |
| Quartile 3 | 68.0 | 24.7 | 7.3 |
| Quartile 4 (highest) | 64.4 | 29.6 | 6.0 |
| Patient residence | |||
| Large metropolitan | 71.4 | 22.3 | 6.2 |
| Small/medium metropolitan | 70.5 | 21.5 | 8.1 |
| Micropolitan/noncore | 67.5 | 23.9 | 8.6 |
| Expected payer | |||
| Medicare | 57.3 | 34.1 | 8.6 |
| Medicaid | 87.0 | 8.0 | 5.0 |
| Private insurance | 63.2 | 29.2 | 7.7 |
| Uninsured | 82.6 | 8.6 | 8.9 |
| Supplemental Table 4. Population rate of opioid-related inpatient stays among women overall and by patient characteristics in 2016 for data presented in Figure 4 | |||
| Characteristic | Rate of opioid-related inpatient stays per 100,000 population | ||
|---|---|---|---|
| All opioid stays | 374.8 | ||
| Age, years | |||
| 15-44 | 332.0 | ||
| 45-64 | 405.0 | ||
| 65+ | 426.7 | ||
| Race/ethnicity | |||
| Black | 379.8 | ||
| Hispanic | 152.2 | ||
| White | 428.3 | ||
| Other | 164.1 | ||
| Community income | |||
| Quartile 1 (lowest) | 484.6 | ||
| Quartile 2 | 398.8 | ||
| Quartile 3 | 335.5 | ||
| Quartile 4 (highest) | 252.2 | ||
| Patient residence | |||
| Large metropolitan | 361.4 | ||
| Small/medium metropolitan | 382.0 | ||
| Micropolitan/noncore | 391.7 | ||
| Supplemental Table 5. Population rate of opioid-related inpatient stays among women by community-level income quartile, patient residence, and race/ethnicity in 2016 for data presented in Figure 5 and Figure 6 | |||||||
| Race/ ethnicity | Rate of stays by community-level income | Rate of stays by location of patient residence | |||||
|---|---|---|---|---|---|---|---|
| Quartile 1(lowest) | Quartile 2 | Quartile 3 | Quartile 4 (highest) | Large metropolitan areas | Medium/small metropolitan areas | Micropolitan/noncore areas | |
| Black | 457.5 | 330.1 | 302.2 | 242.3 | 424.8 | 300.9 | 208.8 |
| Hispanic | 179.2 | 145.6 | 126.1 | 82.6 | 147.7 | 153.0 | 142.9 |
| White | 613.1 | 463.0 | 380.8 | 282.9 | 433.9 | 426.7 | 403.2 |
| Other | 290.7 | 183.5 | 137.0 | 96.1 | 143.3 | 163.2 | 305.5 |
| Internet Citation: Statistical Brief #247. Healthcare Cost and Utilization Project (HCUP). January 2019. Agency for Healthcare Research and Quality, Rockville, MD. hcup-us.ahrq.gov/reports/statbriefs/sb247-Opioid-Hospital-Stays-Women.jsp. |
| Are you having problems viewing or printing pages on this website? |
| If you have comments, suggestions, and/or questions, please contact hcup@ahrq.gov. |
| If you are experiencing issues related to Section 508 accessibility of information on this website, please contact hcup@ahrq.gov. |
| Privacy Notice, Viewers & Players |
| Last modified 1/17/19 |