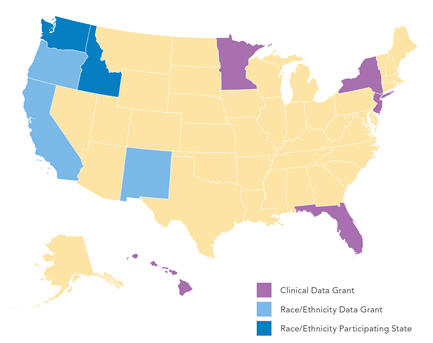
Clinical Content Enhancement
Five grantees broadened and supplemented their existing population-based data with hospital-based electronic pharmacy data, clinical laboratory data, prehospital emergency care data, clinical registries, and vital record birth and death certificates.
Florida
Investigators at the University of South Florida leveraged a strong collaborative partnership among many of Florida�s key healthcare entities to create a statewide enhanced maternal�infant database of clinical and nonclinical information derived from birth and death vital records, as well as inpatient, ambulatory, and emergency department data. The end product was tested by conducting a comparative effectiveness research study using early-term elective delivery as a case study. The database serves as a sustainable tool for research, quality improvement, and enhancement of overall health, and as a model for other states with similar objectives. To date, the Florida project has:
- Expanded existing partnerships and forged new local, state, and national partnerships to foster collaboration around innovative research ideas and improve infrastructure
- Improved data quality with a standardized protocol to process various types of health records, identified errors/inconsistencies in datasets and developed remedies, and identified previously undocumented data decisions
- Implemented unique strategies for linking maternal and child health records from disparate data sources, created a hierarchical linking algorithm, implemented innovative procedures to automate post-linkage processing rules, and improved the ability to link multiple births as well as health records with missing Social Security numbers and names
- Constructed a database for conducting analyses on maternal�child health populations in Florida
- Developed a methodology for calculating reliable cost estimates in administrative data
The Florida team has published timely manuscripts in peer-reviewed journals, including �The Missing Link in Preconceptional Care: The Role of Comparative Effectiveness Research� and �Cutting Edge Technology for Public Health Workforce Training in Comparative Effectiveness Research,� and has participated in numerous panels and presentations based on the work and products of the grant. The team plans to continue collaborating with their current partners, disseminating their findings, and developing methodological documentation for those interested in their data linkage approach. Grant abstract: PDF file, 18 KB; HTML
Hawaii
Collaborators from The Queen�s Medical Center and Hawaii Health Information Consortium have enhanced the clinical content of Hawaii�s statewide hospital discharge database by adding laboratory results, and have furthered development of a master patient identifier to link and track patients across hospitals throughout the state. The researchers demonstrated the viability of the enhanced database by performing a comparative effectiveness research study to examine the outcomes of care for patients treated by hospitalists compared with patients treated by nonhospitalists. The end result will be an enduring infrastructure that will improve research and quality. The Hawaii grant has:
- Forged relationships with and secured participation of Hawaii�s hospitals and laboratories
- Installed a Health Level Seven interface engine and designed protocols to accept data from disparate hospital systems. The team is now receiving production data feeds from all major non-federal hospitals in the state.
- Successfully linked laboratory data to hospital discharge data
- Established a Master Patient ID (including newborns) allowing patient-level tracking across level of service and between providers
The Hawaii team continues to assess and improve data quality, and to conduct research to measure the value of clinically enhanced data to improve risk models and analytical models to better predict hospital outcomes such as readmissions, mortality, and inpatient complications. Grant abstract: PDF file, 16 KB; HTML
Minnesota
The Minnesota Hospital Association (MHA), in collaboration with Michael Pine Associates and the Mayo Clinic Division of Health Care Policy and Research, has augmented the current MHA clinically enhanced administrative hospital discharge database with laboratory data from additional hospitals, and introduced hospital pharmacy data and Minnesota death certificate data to the database. The end goal of the project was to use these data to facilitate rich comparative effectiveness analysis and to enhance the scope and quality of the Minnesota hospital discharge database. The project has:
- Increased hospital enrollment in the project with 25 hospitals currently submitting data, with a total of 30 hospitals enrolled
- Designed specifications, database edits, and layouts; and tested hospital data files
- Installed a Health Level Seven healthcare integration engine to facilitate compilation of study data
- Developed hospital reports on data quality (including present-on-admission and congestive heart failure cases), individual recommendations about the pharmacological management of ADHF (Acute Decompensated Heart Failure) patients, and risk-adjusted clinical outcomes comparing other participating hospitals
Going forward, the research team intends to expand their laboratory database to include more hospitals, evaluate creating new quality reports based on the findings of the data, and continue proving the business case for hospital participation. Grant abstract: PDF file, 10 KB; HTML. Website: Minnesota AHRQ Lab Project New Jersey
New Jersey
An innovative partnership between academic researchers at Rutgers Center for State Health Policy and the New Jersey Department of Health and Senior Services has created a data infrastructure that bridges prehospital and hospital care using electronic patient care records for emergency medical services transports in New Jersey. These data linked all-payer hospital discharge data and death certificates to support a wide range of studies on interventions that involve prehospital and hospital services. A comparative effectiveness study of outcomes after provision of therapeutic hypothermia for initial survivors of out-of-hospital cardiac arrest has illustrated the value of the data. The project has:
- Created a fully linked database for the years 2009 to 2010 and worked with local emergency services to better understand the varied procedural issues that affect the data
- Produced a detailed report on their data linkage methods which has been posted on the Rutgers Center for State Health Policy website
- Completed a survey of therapeutic hypothermia availability and delivery protocols at all New Jersey hospitals. Findings have been disseminated in the journal Therapeutic Hypothermia and Temperature Management, at the AcademyHealth Meeting and New Jersey Cardiovascular Health Advisory Panel. Additional analyses are currently under peer review.
The New Jersey team plans to complete linkage for years 2011�2012 and continue dissemination of findings through various outlets. The grant work has afforded the New Jersey team the opportunity to participate in several panels and presentations. Grant abstract: PDF file, 16 KB; HTML
New York
The New York State (NYS) Department of Health; School of Public Health, SUNY-Albany; and Michael Pine Associates have worked together to link administrative data from NYS� Statewide Planning and Research Cooperative System (SPARCS) acute care hospital discharge database to laboratory test results from facilities that perform coronary artery bypass graft (CABG) surgery or elective percutaneous coronary interventions (PCI). To assess the value of the resulting clinically enhanced database, the research team has compared comparative risk-adjusted outcomes and analyses of the appropriateness of alternative revascularization procedures using the clinically enhanced administrative database with analyses performed using specialized CABG and PCI registries. Another goal of the project was to determine whether laboratory test results will enhance the ability of the cardiac registry data to risk-adjust patient outcomes. The project has reached a number of milestones:
- Data Use Agreements have been approved for all major data sources used in the study.
- The New York State Health Commissioner has designated the project a research study governed by NYS Public Law 206 (1) (j), an important distinction that protects hospital participants� confidentiality.
- Successful record matching has been accomplished on 3 years of SPARCS, cardiac, PCI, and vital records data.
- Twenty of 56 eligible New York hospitals have been recruited to participate in the study and have supplied required laboratory data. Laboratory data have been reviewed for completeness and validity.
- Data from all 20 hospitals have been judged satisfactory for analysis. Matches of laboratory data to SPARCS data are being conducted after laboratory data pass quality reviews.
The New York team conducted analyses that compared outcome measures, risk-adjustment models, comparative hospital performance, and decision making; explored the effects of data enhancements on predictive variable, risk-adjustment, and propensity models; described differences in results of comparable analyses using alternative data sets; identified the most cost-effective methods of creating databases for performance monitoring and comparative effectiveness studies; and plans to disseminate findings, conclusions, lessons learned, and tools for future use. Grant abstract: PDF file, 16 KB; HTML
|
Race and Ethnicity Data Improvement
Three grantees improved the validity, reliability, and detail of patient race and ethnicity data which will generate better data for comparative effectiveness research to improve healthcare outcomes, including less disparate outcomes for different racial and ethnic groups.
California
Investigators from the University of California, Los Angeles, in collaboration with the California Office of Statewide Health Planning and Development (OSHPD) improved the reliability, validity, and completeness of self-reported race, ethnicity, and primary language (R/E/L) provided by hospitals in three OSHPD databases. The project has assessed data collection, reporting, and accuracy in California hospitals; benchmarked the data against six comparison states; and will improve hospital R/E/L data via development of standardized materials, educational intervention, auditing, and follow-up. The researchers have linked OSHPD databases to other state agency data and used statistical approaches to authenticate their efforts. The project has made substantial, sustainable improvements to the reporting of R/E/L among patients in California�s hospitals. The project has:
- Performed a baseline assessment of R/E/L data collection, reporting, and accuracy among acute care hospitals in California and shared hospital survey results at professional conferences
- Created and disseminated tools to improve quality and consistency of collection of R/E/L data targeted to hospitals
- Developed candidate audit measures to estimate improved R/E/L reporting
- Conducted three webinars for more than 350 hospital representatives throughout California
- Linked OSHPD�s inpatient, emergency department, and ambulatory surgery data to data from cancer registries and cancer clinical trials (considered the "gold standard" for R/E/L accuracy)
Going forward, the California team will continue revising audit measures; apply supplemental data and statistical methods to improve data completeness; perform a follow-up of California hospital practices, attitudes, and performance; and utilize strategies to convince hospitals of the importance of improving R/E/L data collection. Grant abstract: PDF file, 16 KB; HTML. Website: Improving Race, Ethnicity, and Language Collection in California
New Mexico
The New Mexico Department of Health has improved the quality of race and ethnicity data in hospital discharge databases by revising the New Mexico administrative code to mandate race, ethnicity, and tribal identifier data reporting. Specific goals of the grant project included: improving patient race and ethnicity data in the New Mexico Hospital Inpatient Discharge Data; collecting tribal identifier data; evaluating the quality of race and ethnicity data; and sharing methods, tools, and procedures with other states. The project has:
- Changed state regulations to align with 1997 U.S. Office of Management and Budget standards
- Developed a systematic method to identify and target institutional factors influencing data collection
- Increased awareness of the need to improve data quality at the hospital level through presentations and webinars
- Produced hospital training materials including FAQ sheets, PowerPoint presentations, informational sheets, pre/post training tests, and key informant surveys
- Conducted a patient telephone survey to measure quality improvement in race data collected post-hospital training
The New Mexico team has begun to realize an increase in data quality across all targeted fields. The work related to this grant has afforded New Mexico the opportunity to disseminate findings at various venues, including national conferences, meetings, webinars, peer-reviewed journals, and the New Mexico Health Information Technology website. Grant abstract: PDF file, 10 KB; HTML. Website: New Mexico Health Information Technology
Oregon/Washington/Idaho
Using the most complete roster of Northwest American Indian/Alaska Native (AI/AN) people available, the Improving Data & Enhancing Access-Northwest (IDEA-NW) Project of the Northwest Portland Area Indian Health Board has conducted record linkages with an array of health-related data systems in a three-state region to identify and, in some cases, augment racial misclassification and improve disease/mortality estimates. The project has:
- Identified racial misclassification in hospital discharge systems (Oregon and Washington), cancer registries (three states), death certificates (three states), birth certificates (Oregon and Idaho), Medicaid (Oregon), STD/HIV/CD (Oregon and Idaho), childhood blood lead registry (Oregon), and trauma registries (Washington and Idaho)
- Engaged in meaningful discussion with state data managers about race data quality and usefulness of their surveillance systems for minority health assessment. Several partners have implemented rules to correct race classification of AI/AN people based on linkage findings.
- Generated state-level health reports on AI/AN mortality, cancer, maternal and child health, and blood levels
- Generated tribe-level cancer data reports for 43 Northwest Tribes
- Completed assessment of the Northwest Tribal Registry linkage dataset
- Greatly improved collaboration between the Tribal Epidemiology Center and the Departments of Health in Idaho, Oregon, and Washington, and with organizations that serve urban Indians in the Northwest
- Disseminated results through peer-reviewed journals, reports, national conferences, meetings, and the IDEA-NW website.
The researchers plan to continue conducting linkages to improve race classification for AI/AN in the three states, and disseminating findings through local and state-level reports. They also plan to continue developing concrete methods by which other states and Tribal Epidemiology Centers can implement similar programs. Grant abstract: PDF file, 17 KB; HTML. Website: NPAIHB IDEA-NW
|