|
STATISTICAL BRIEF #288
February 2022
Kathryn R. Fingar, Ph.D., M.P.H., and Marc Roemer, M.S. Introduction In 2019, approximately one in five adults in the United States reported having some type of mental illness in the past year, and 16 percent of these adults received mental health services.1 Mental disorders are a leading reason for hospitalization in the United States.2 Depressive disorders and schizophrenia rank in the top 20 principal diagnoses for inpatient stays.2,3 Rates of inpatient stays for mental disorders reflect many factors, including the prevalence of mental disorders in the community, the availability of treatment options, as well as access to treatment. Inpatient stays for mental disorders are especially important to track at the substate level to inform inpatient and outpatient resource allocation based on the needs of the community. Statistics from 2016-2018 provide a baseline from which to examine changes in inpatient utilization for mental disorders that have occurred since the beginning of the COVID-19 pandemic in 2020.4 This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents 3-year aggregate statistics on national, State, and substate regional variation in inpatient stays for mental disorders among patients of all ages at community hospitals (excluding rehabilitation and long-term care hospitals) based on the 2016-2018 National Inpatient Sample (NIS) and the 2016-2018 State Inpatient Databases (SID). Geographic areas are based on the patient ZIP Code of residence. This Statistical Brief focuses on the five leading mental disorder principal diagnoses for inpatient stays in the United States: depressive disorders, schizophrenia spectrum and other psychotic disorders, bipolar and related disorders, suicidal ideation or attempt and intentional self-harm, and trauma- and stressor-related disorders. Statistics are presented for 38 States that, at the time this Statistical Brief was written, had released aggregate 2016-2018 data through the Community-Level Statistics path of HCUPnet, an online query tool for county- and substate region-level statistics.2 These States represented 80 percent of the U.S. population in 2018. Because of the large sample size of the NIS and SID data, small differences can be statistically significant but not clinically important. Thus, only differences greater than or equal to 10 percent are discussed in the text. Findings State variation in the rate of inpatient stays for mental disorders, 2016-2018 Figure 1 illustrates the distribution (i.e., minimum and maximum values as well as the 25th and 75th percentiles) of population rates of the five leading mental disorder reasons (i.e., principal diagnosis) for inpatient stays across the 38 States included in this Statistical Brief. The national rate also is presented. |
|
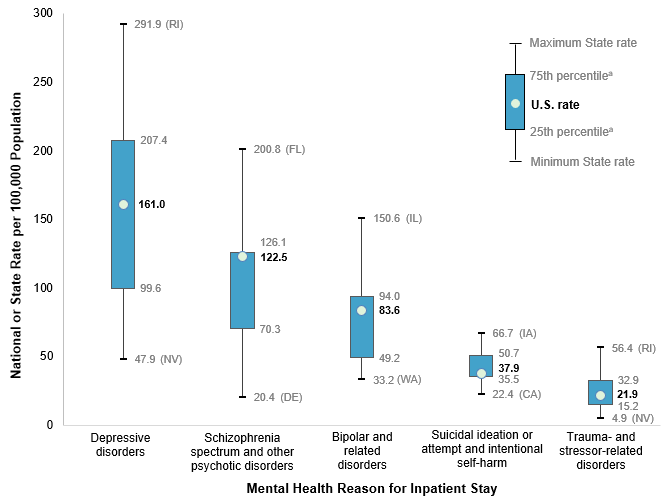
Figure 1. Variation in State rate (per 100,000 population) of leading mental disorder principal diagnoses for inpatient stays, 2016-2018
a The 25th and 75th percentiles are based on the distribution of rates across the 38 States that participate in the HCUPnet Community-Level Statistics path. The U.S. rate is a national weighted estimate from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS). Box and whisker plot showing the distribution (i.e., minimum and maximum values as well as the 25th and 75th percentiles) of population rates of the five leading mental disorder reasons for inpatient stays across 38 States as well as the national rate. Depressive disorders: minimum State rate, 47.9 (NV); 25th percentile, 99.6; U.S. rate, 161.0; 75th percentile, 207.4; maximum State rate, 291.9 (RI). Schizophrenia spectrum and other psychotic disorders: minimum State rate, 20.4 (DE); 25th percentile, 70.3; U.S. rate, 122.5; 75th percentile, 126.1; maximum State rate, 200.8 (FL). Bipolar and related disorders: minimum State rate, 33.2 (WA); 25th percentile, 49.2; U.S. rate, 83.6; 75th percentile, 94.0; maximum State rate, 150.6 (IL). Suicidal ideation or attempt and intentional self-harm: minimum State rate, 22.4 (CA); 25th percentile, 35.5; U.S. rate, 37.9; 75th percentile, 50.7; maximum State rate, 66.7 (IA). Trauma- and stressor-related disorders: minimum State rate, 4.9 (NV); 25th percentile, 15.2; U.S. rate, 21.9; 75th percentile, 32.9; maximum State rate, 56.4 (RI).
|
| Table 1. Rate of inpatient stays per 100,000 population of the top five mental disorder principal diagnoses and State rank, 2016-2018 | ||||||||||
| State | Depressive disorders | Schizophrenia spectrum and other psychotic disorders | Bipolar and related disorders | Suicidal ideation or attempt and intentional self-harm | Trauma- and stressor-related disorders | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Rate | State rank | Rate | State rank | Rate | State rank | Rate | State rank | Rate | State rank | |
| United States | 161.0 | — | 122.5 | — | 83.6 | — | 37.9 | — | 21.9 | — |
| Alaska | 137.2 | 27 | 66.3 | 31 | 41.6 | 35 | 61.8 | 4 | 33.0 | 10 |
| Arizona | 63.7 | 36 | 58.7 | 32 | 47.1 | 30 | 36.8 | 27 | 13.1 | 30 |
| Arkansas | 196.7 | 13 | 143.2 | 6 | 79.8 | 19 | 63.1 | 3 | 34.7 | 8 |
| California | 70.3 | 34 | 147.5 | 4 | 43.1 | 34 | 22.4 | 38 | 7.7 | 37 |
| Colorado | 80.7 | 32 | 42.7 | 37 | 35.9 | 37 | 40.7 | 20 | 19.3 | 22 |
| Delaware | 67.0 | 35 | 20.4 | 38 | 37.4 | 36 | 35.4 | 29 | 7.9 | 36 |
| Florida | 197.0 | 12 | 200.8 | 1 | 109.1 | 8 | 41.4 | 18 | 32.3 | 11 |
| Georgia | 87.3 | 31 | 95.0 | 21 | 51.8 | 27 | 31.5 | 33 | 11.0 | 32 |
| Hawaii | 97.4 | 29 | 91.9 | 23 | 49.3 | 28 | 24.8 | 37 | 29.9 | 13 |
| Illinois | 235.5 | 6 | 173.2 | 2 | 150.6 | 1 | 39.9 | 24 | 15.7 | 28 |
| Indiana | 232.8 | 7 | 99.9 | 18 | 84.4 | 16 | 40.6 | 21 | 18.3 | 24 |
| Iowa | 242.9 | 4 | 95.4 | 20 | 87.5 | 14 | 66.7 | 1 | 37.2 | 7 |
| Kentucky | 208.9 | 10 | 96.4 | 19 | 70.0 | 22 | 43.9 | 17 | 30.7 | 12 |
| Louisiana | 175.4 | 21 | 139.9 | 7 | 92.3 | 13 | 32.7 | 32 | 20.8 | 20 |
| Maryland | 190.0 | 16 | 126.6 | 10 | 128.8 | 4 | 25.0 | 36 | 22.6 | 19 |
| Massachusetts | 178.6 | 20 | 105.5 | 15 | 93.6 | 11 | 39.8 | 25 | 38.8 | 5 |
| Michigan | 146.7 | 26 | 92.1 | 22 | 87.5 | 15 | 45.2 | 16 | 15.1 | 29 |
| Minnesota | 242.9 | 5 | 124.5 | 11 | 84.4 | 17 | 58.6 | 6 | 45.5 | 3 |
| Mississippi | 184.2 | 18 | 134.6 | 8 | 66.5 | 24 | 35.7 | 28 | 54.4 | 2 |
| Montana | 202.8 | 11 | 83.6 | 24 | 84.3 | 18 | 64.2 | 2 | 43.9 | 4 |
| Nebraska | 276.9 | 2 | 128.1 | 9 | 140.4 | 2 | 45.7 | 15 | 34.5 | 9 |
| Nevada | 47.9 | 38 | 104.2 | 17 | 68.7 | 23 | 40.3 | 22 | 4.9 | 38 |
| New Jersey | 175.2 | 22 | 145.8 | 5 | 121.7 | 6 | 28.4 | 35 | 19.2 | 23 |
| New Mexico | 179.8 | 19 | 105.1 | 16 | 92.5 | 12 | 48.3 | 14 | 18.1 | 25 |
| North Carolina | 196.4 | 14 | 110.7 | 14 | 94.2 | 10 | 32.7 | 31 | 24.0 | 16 |
| North Dakota | 193.2 | 15 | 68.7 | 29 | 65.2 | 25 | 50.1 | 11 | 38.0 | 6 |
| Oklahoma | 147.3 | 25 | 80.0 | 27 | 71.0 | 21 | 60.9 | 5 | 11.5 | 31 |
| Oregon | 77.7 | 33 | 82.0 | 25 | 49.1 | 29 | 52.7 | 8 | 16.3 | 27 |
| Pennsylvania | 215.3 | 9 | 121.0 | 12 | 117.2 | 7 | 41.0 | 19 | 27.7 | 15 |
| Rhode Island | 291.9 | 1 | 168.5 | 3 | 127.6 | 5 | 49.5 | 12 | 56.4 | 1 |
| South Carolina | 106.2 | 28 | 75.2 | 28 | 46.0 | 31 | 38.7 | 26 | 22.8 | 17 |
| Tennessee | 188.9 | 17 | 81.8 | 26 | 98.7 | 9 | 39.9 | 23 | 16.7 | 26 |
| Texas | 93.4 | 30 | 55.5 | 35 | 45.0 | 32 | 31.3 | 34 | 9.7 | 34 |
| Utah | 229.7 | 8 | 68.3 | 30 | 74.2 | 20 | 50.9 | 10 | 10.1 | 33 |
| Washington | 55.2 | 37 | 55.7 | 34 | 33.2 | 38 | 33.7 | 30 | 9.7 | 35 |
| West Virginia | 270.8 | 3 | 119.9 | 13 | 139.7 | 3 | 51.3 | 9 | 22.8 | 18 |
| Wisconsin | 167.4 | 23 | 56.5 | 33 | 58.1 | 26 | 49.0 | 13 | 20.6 | 21 |
| Wyoming | 147.8 | 24 | 43.1 | 36 | 45.0 | 33 | 56.7 | 7 | 29.4 | 14 |
| Notes: Rates are per 100,000 population. The U.S. rate is a national weighted estimate from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS). Source: Agency for Healthcare Research and Quality (AHRQ), Healthcare Cost and Utilization Project (HCUP), 2016-2018 National Inpatient Sample (NIS) and 2016-2018 State Inpatient Databases (SID) for 38 States that, at the time this Statistical Brief was written, had released aggregate 2016-2018 data through the Community-Level Statistics path on HCUPnet, an online query tool | ||||||||||
Figures 2 through 6 display rates of the five most common mental disorder reasons for inpatient stays by substate region. The rates are categorized into quintiles based on the distribution of unsuppressed rates across all regions in the 38 States included in this Statistical Brief. Within these States, there are 255 substate regions identified by Community-Level Statistics. Hot spots were defined as regions with rates in the highest quintile (quintile 5). |
|
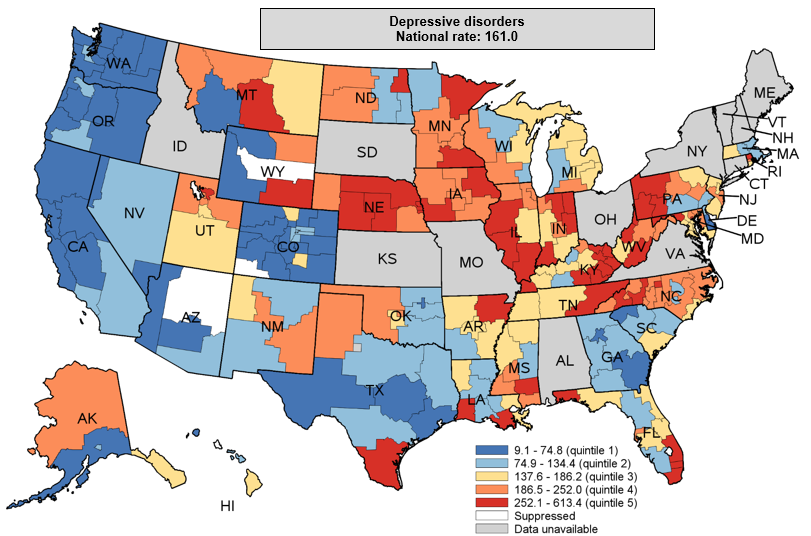
Figure 2. Rate of inpatient stays with a principal diagnosis of depressive disorders per 100,000 population, by substate region, 2016-2018
Note: Data for Hawaii and Delaware are at the county level, not the substate region level. The quintiles are based on the distribution of unsuppressed rates across the 38 States that participate in the HCUPnet Community-Level Statistics path. The U.S. rate is a national weighted estimate from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS). Color-coded map of the United States that shows substate region-level rates per 100,000 population for inpatient stays with a principal diagnosis of depressive disorders in 2016 to 2018 for 38 States, by rate quintile (quintile 1: 9.1-74.8; quintile 2: 74.9-134.4; quintile 3: 137.6-186.2; quintile 4: 186.5-252.0; quintile 5: 252.1-613.4). National rate: 161.0.
|
|
|
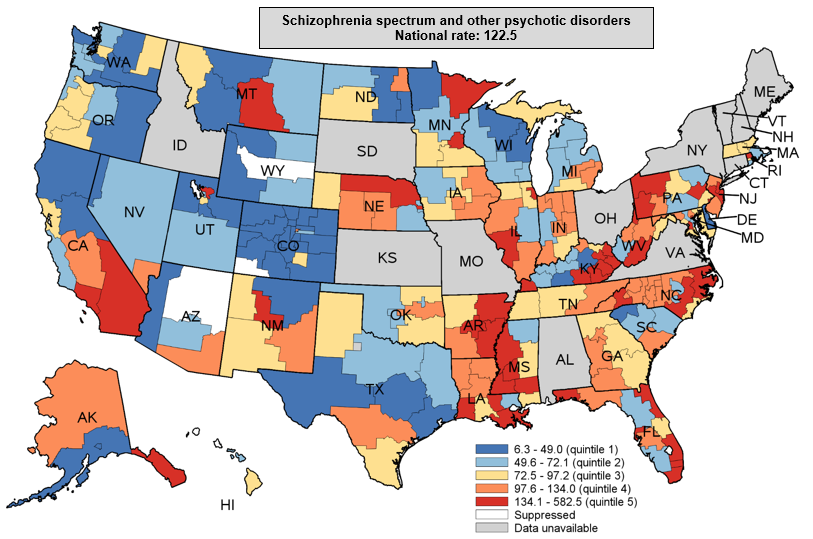
Figure 3. Rate of inpatient stays with a principal diagnosis of schizophrenia spectrum and other psychotic disorders per 100,000 population, by substate region, 2016-2018
Note: Data for Hawaii and Delaware are at the county level, not the substate region level. The quintiles are based on the distribution of unsuppressed rates across the 38 States that participate in the HCUPnet Community-Level Statistics path. The U.S. rate is a national weighted estimate from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS). Color-coded map of the United States that shows substate region-level rates per 100,000 population for inpatient stays with a principal diagnosis of schizophrenia spectrum and other psychotic disorders in 2016 to 2018 for 38 States, by rate quintile (quintile 1: 6.3-49.0; quintile 2: 49.6-72.1; quintile 3: 72.5-97.2; quintile 4: 97.6-134.0; quintile 5: 134.1-582.5). National rate: 122.5.
|
|
|
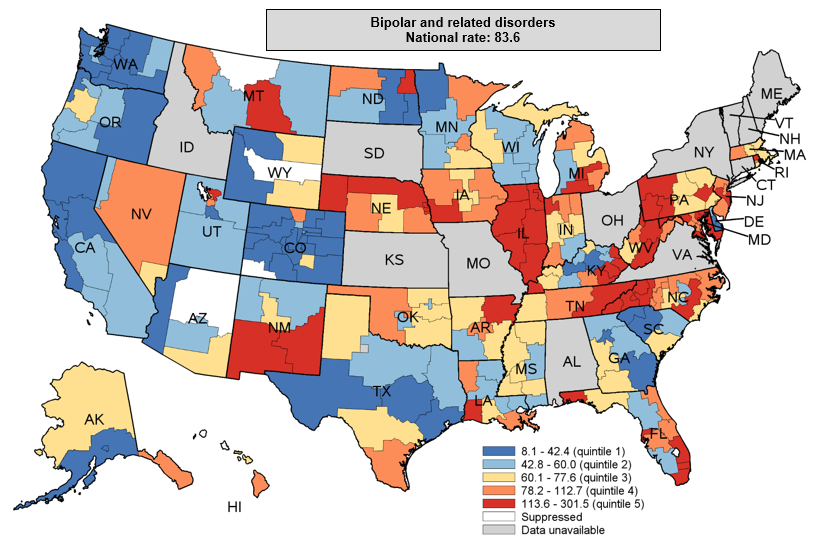
Figure 4. Rate of inpatient stays with a principal diagnosis of bipolar and related disorders per 100,000 population, by substate region, 2016-2018
Note: Data for Hawaii and Delaware are at the county level, not the substate region level. The quintiles are based on the distribution of unsuppressed rates across the 38 States that participate in the HCUPnet Community-Level Statistics path. The U.S. rate is a national weighted estimate from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS). Color-coded map of the United States that shows substate region-level rates per 100,000 population for inpatient stays with a principal diagnosis of bipolar and related disorders in 2016 to 2018 for 38 States, by rate quintile (quintile 1: 8.1-42.4; quintile 2: 42.8-60.0; quintile 3: 60.1-77.6; quintile 4: 78.2-112.7; quintile 5: 113.6-301.5). National rate: 83.6.
|
|
|
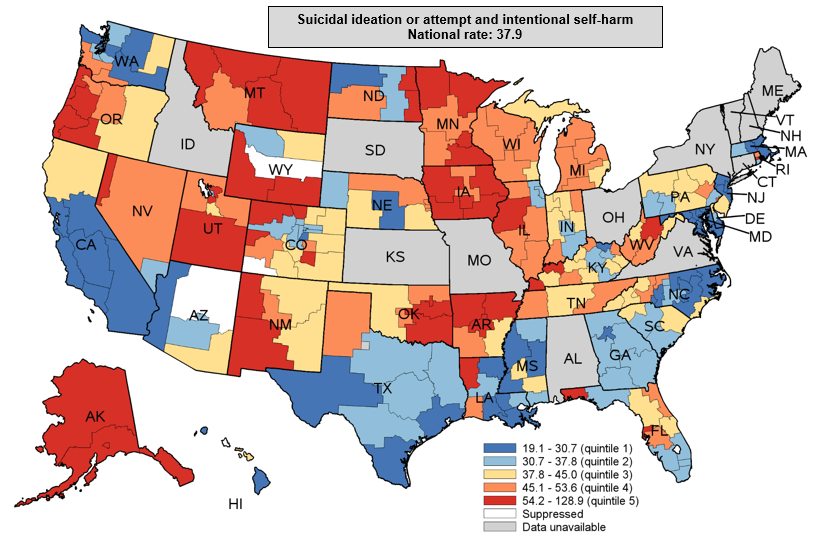
Figure 5. Rate of inpatient stays with a principal diagnosis of suicidal ideation or attempt and intentional self-harm per 100,000 population, by substate region, 2016-2018
Note: Data for Hawaii and Delaware are at the county level, not the substate region level. The quintiles are based on the distribution of unsuppressed rates across the 38 States that participate in the HCUPnet Community-Level Statistics path. The U.S. rate is a national weighted estimate from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS). Color-coded map of the United States that shows substate region-level rates per 100,000 population for inpatient stays with a principal diagnosis of suicidal ideation or attempt and intentional self-harm in 2016 to 2018 for 38 States, by rate quintile (quintile 1: 19.1-30.7; quintile 2: 30.7-37.8; quintile 3: 37.8-45.0; quintile 4: 45.1-53.6; quintile 5: 54.2-128.9). National rate: 37.9.
|
|
|
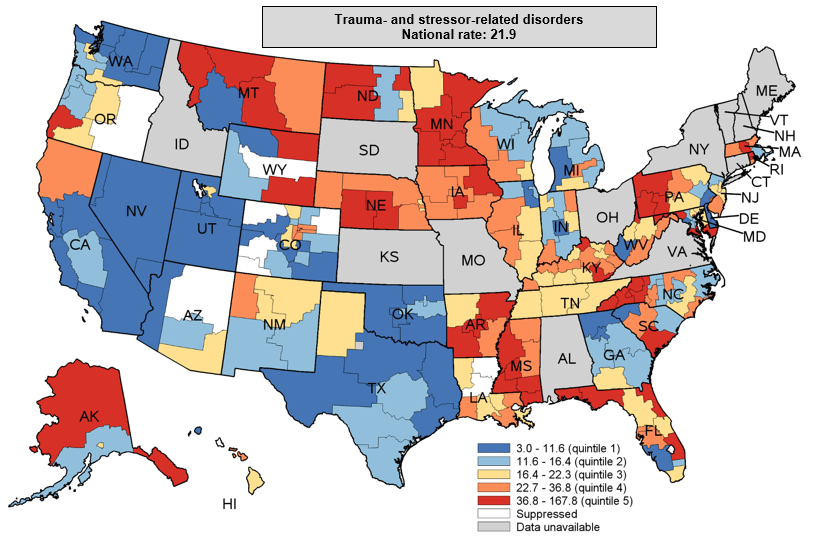
Figure 6. Rate of inpatient stays with a principal diagnosis of trauma- and stressor-related disorders per 100,000 population, by substate region, 2016-2018
Note: Data for Hawaii and Delaware are at the county level, not the substate region level. The quintiles are based on the distribution of unsuppressed rates across the 38 States that participate in the HCUPnet Community-Level Statistics path. The U.S. rate is a national weighted estimate from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS). Color-coded map of the United States that shows substate region-level rates per 100,000 population for inpatient stays with a principal diagnosis of trauma- and stressor-related disorders in 2016 to 2018 for 38 States, by rate quintile (quintile 1: 3.0-11.6; quintile 2: 11.6-16.4; quintile 3: 16.4-22.3; quintile 4: 22.7-36.8; quintile 5: 36.8-167.8). National rate: 21.9.
|
|