STATISTICAL BRIEF #254 |
October 2019
Anita Soni, Ph.D., M.B.A., Kathryn R. Fingar, Ph.D., M.P.H., and Lawrence D. Reid, Ph.D., M.P.H. Introduction In 2016 in the United States, approximately 20.1 million people aged 12 years or older had a substance use disorder (SUD) in the past year.1 Higher rates of SUDs are reported by individuals between the ages of 18 and 25 years.2 Thus, many women with an SUD are of reproductive age. In 2016, 6 percent of pregnant women reported illicit drug use and 8 percent reported alcohol use.3 Substance use during pregnancy is associated with specific risks for mothers and their infants. Other than cannabis, opioids and cocaine are the most common types of substance use diagnosed at delivery.4 Opioid use during pregnancy may lead to neonatal abstinence syndrome (NAS), which is a constellation of signs and symptoms most commonly caused by abrupt cessation of prescription or illegal opioids at birth following repeated prenatal exposure.5 Infants with NAS often have fussiness, breathing problems, difficulty feeding, and poor weight gain.6 Babies born to mothers who use opioids or stimulants during pregnancy are often born prematurely and with low birth weights.7,8 The long-term care for these infants is very costly to hospitals and families. Use of cocaine and other stimulants during pregnancy can cause maternal migraines and seizures, as well as exacerbate cardiovascular changes during pregnancy, leading to hypertensive crises9 and potentially to postpartum mortality.10 Compared with urban areas, rates of substance use during pregnancy are frequently higher in rural areas, which often have limited resources for prevention and treatment.11,12 For instance, rates of opioid prescriptions are higher in rural than in urban areas13 and prescription opioids are now the most common type of drug abused by rural pregnant women.14 Despite these statistics, most research on the prevalence, prevention, and treatment of substance abuse during pregnancy has been conducted in urban areas.15 This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents statistics from the 2016 National Inpatient Sample (NIS) on delivery-related inpatient stays involving SUDs, overall and for select types of substances: opioids, cocaine, and other stimulants, as well as for both urban and rural areas. The definition of any substance use does not include tobacco use. Clinical outcomes at delivery are examined, including preterm delivery (birth before 37 weeks of gestation), severe pre-eclampsia/eclampsia (a condition marked by high blood pressure, protein in the urine, and/or organ dysfunction, which can progress to the onset of seizures), obstetric hemorrhage/placenta accreta (a condition in which the placenta grows too deeply into the uterine wall, causing severe blood loss after delivery), and placental abruption (early separation of the placenta from the uterus). These outcomes are compared across deliveries with and without an SUD diagnosis and by urban or rural location of the patient's residence. Because of the large sample size of the HCUP NIS, small differences can be statistically significant. Thus, only differences between groups greater than or equal to 10 percent are noted in the text. |
|
Findings
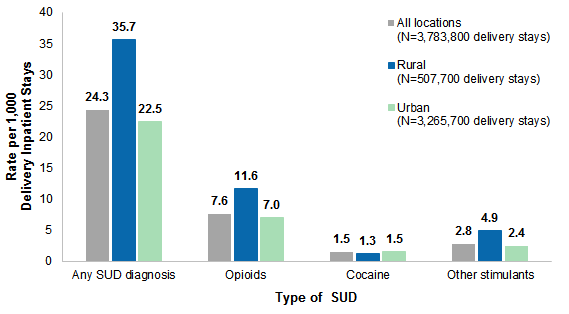
Rates of delivery inpatient stays involving SUDs, 2016 Figure 1 displays the rate of deliveries involving SUDs per 1,000 total delivery stays among patients who resided in rural versus urban counties in 2016. The rate is presented overall and for select types of SUD diagnoses. |
|
Figure 1. Rates of delivery stays involving SUDs among patients residing in rural versus urban counties, overall and for select types of SUD diagnoses, 2016
Abbreviation: SUD, substance use disorder Bar chart that shows the rate per 1,000 delivery inpatient stays by type of SUD diagnosis for patients who reside in rural and urban counties in 2016. Data are provided in Supplemental Table 1.
|
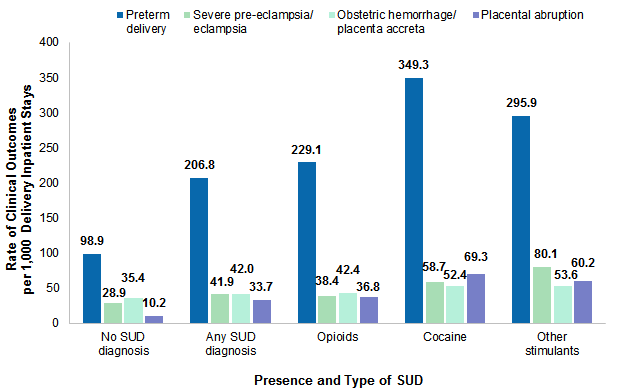
Figure 2 displays the rate of deliveries with select clinical outcomes per 1,000 delivery stays involving SUDs in 2016, compared with deliveries with no SUD diagnosis. Rates are shown for delivery stays with any SUD diagnosis and for deliveries involving specific types of substances. |
|
Figure 2. Comparison of clinical outcomes among delivery stays with and without an SUD diagnosis, 2016
Abbreviation: SUD, substance use disorder Bar chart that shows the rate of clinical outcomes per 1,000 delivery inpatient stays by presence and type of SUD diagnosis in 2016. Data are provided in Supplemental Table 2.
|
|
| Table 1. Comparison of clinical outcomes among delivery stays with and without an SUD diagnosis, by location of patient residence, 2016 | |||||
| Location of patient residence and clinical outcomes | SUD type | ||||
|---|---|---|---|---|---|
| No SUD diagnosis | Any SUD diagnosis | Opioids | Cocaine | Other stimulants | |
| Urban | |||||
| Total delivery inpatient stays, N | 3,192,300 | 73,400 | 22,800 | 4,900 | 8,000 |
| Rate of clinical outcomes per 1,000 delivery stays | |||||
| Preterm delivery | 98.2 | 209.1 | 239.6 | 354.3 | 298.8 |
| Severe pre-eclampsia/eclampsia | 29.2 | 44.3 | 41.2 | 59.7 | 86.6 |
| Placenta accreta/postpartum hemorrhage | 35.8 | 42.4 | 42.8 | 56.7 | 55.9 |
| Placental abruption | 10.2 | 31.7 | 35.7 | 69.8 | 59.0 |
| Rural | |||||
| Total delivery inpatient stays, N | 489,600 | 18,100 | 5,900 | 600 | 2,500 |
| Rate of clinical outcomes per 1,000 delivery stays | |||||
| Preterm delivery | 103.6 | 195.0 | 187.4 | 299.2 | 278.8 |
| Severe pre-eclampsia/eclampsia | 27.0 | 31.8 | 27.1 | 47.2 | 58.6 |
| Placenta accreta/postpartum hemorrhage | 33.3 | 40.9 | 41.6 | 23.6 | 48.5 |
| Placental abruption | 10.5 | 41.4 | 41.6 | 70.9 | 62.6 |
| Abbreviation: SUD, substance use disorder Notes: Numbers were rounded to the nearest hundred. Rates are based on unrounded values. Source: Agency for Healthcare Research and Quality (AHRQ), Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2016 | |||||
Healthcare Cost and Utilization Project (HCUP) Statistical Briefs provide basic descriptive statistics on a variety of topics using HCUP administrative healthcare data. Topics include hospital inpatient, ambulatory surgery, and emergency department use and costs, quality of care, access to care, medical conditions, procedures, and patient populations, among other topics. The reports are intended to generate hypotheses that can be further explored in other research; the reports are not designed to answer in-depth research questions using multivariate methods. Data Source The estimates in this Statistical Brief are based upon data from the HCUP 2016 National Inpatient Sample (NIS). Definitions Diagnoses, procedures, ICD-10-CM/PCS, and diagnosis-related groups (DRGs) The principal diagnosis is that condition established after study to be chiefly responsible for the patient's admission to the hospital. Secondary diagnoses are concomitant conditions that coexist at the time of admission or develop during the stay. All-listed diagnoses include the principal diagnosis plus these additional secondary conditions. All-listed procedures include all procedures performed during the hospital stay, whether for definitive treatment or for diagnostic or exploratory purposes. The first-listed procedure is the procedure that is listed first on the discharge record. Inpatient data define this as the principal procedure—the procedure that is performed for definitive treatment rather than for diagnostic or exploratory purposes (i.e., the procedure that was necessary to take care of a complication). ICD-10-CM/PCS is the International Classification of Diseases, Tenth Revision, Clinical Modification/Procedure Coding System. In October 2015, ICD-10-CM/PCS replaced the ICD-9-CM diagnosis and procedure coding system with the ICD-10-CM diagnosis coding system for most inpatient and outpatient medical encounters and the ICD-10-PCS procedure coding system for inpatient hospital procedures. There are over 70,000 ICD-10-CM diagnosis codes. There are over 75,000 ICD-10-PCS procedure codes. DRGs comprise a patient classification system that categorizes patients into groups that are clinically coherent and homogeneous with respect to resource use. DRGs group patients according to diagnosis, type of treatment (procedure), age, and other relevant criteria. Each hospital stay has one assigned DRG. Case definition The ICD-10-CM/PCS and DRG codes defining deliveries, substance use disorders (SUDs), and the clinical outcomes examined are provided in Table 2. Note that deliveries were excluded if they had any code indicating an abortive outcome. ICD-10-CM/PCS codes can be up to 7 digits in length. If fewer digits are listed, it indicates that any value in a subsequent position was included, except for the poisoning-related codes (i.e., T-codes). Poisonings included all codes in the series except for underdosing (sixth digit equal to 6) and sequela (seventh digit equal to S). |
| Table 2. Codes defining deliveries, substance use disorders, and clinical outcomes | ||
| Code Type | Code | Description |
|---|---|---|
| Deliveries | ||
| ICD-10-CM | Z37 | Outcome of delivery |
| ICD-10-CM | O80 | Encounter for full-term uncomplicated delivery |
| ICD-10-CM | O82 | Encounter for cesarean delivery without indication |
| DRG | 765 | Cesarean section with complicating conditions/major complicating conditions |
| DRG | 766 | Cesarean section without complicating conditions/major complicating conditions |
| DRG | 767 | Vaginal delivery with sterilization and/or dilation and curettage |
| DRG | 768 | Vaginal delivery with operating room procedure except for sterilization and/or dilation and curettage |
| DRG | 774 | Vaginal delivery with complicating diagnoses |
| DRG | 775 | Vaginal delivery without complicating diagnoses |
| ICD-10-PCS | 10D00Z | Extraction of products of conception, open approach |
| ICD-10-PCS | 10D07Z | Extraction of products of conception, via natural or artificial opening |
| Abortive outcomes | ||
| ICD-10-CM | O00 | Ectopic pregnancy |
| ICD-10-CM | O01 | Hydatidiform mole |
| ICD-10-CM | O02 | Other abnormal products of conception |
| ICD-10-CM | O03 | Spontaneous abortion |
| ICD-10-CM | O04 | Complications following (induced) termination of pregnancy |
| ICD-10-CM | O07 | Failed attempted termination of pregnancy |
| ICD-10-CM | O08 | Complications following ectopic and molar pregnancy |
| ICD-10-CM | 10A0 | Abortion of products of conception |
| Opioids | ||
| ICD-10-CM | F111 | Opioid abuse |
| ICD-10-CM | F112 | Opioid dependence |
| ICD-10-CM | F119 | Opioid use, unspecified |
| ICD-10-CM | T400a | Poisoning by and adverse effect of opium |
| ICD-10-CM | T401a | Poisoning by and adverse effect of heroin |
| ICD-10-CM | T402a | Poisoning by and adverse effect of other opioids |
| ICD-10-CM | T403a | Poisoning by and adverse effect of methadone |
| ICD-10-CM | T404a | Poisoning by and adverse effect of synthetic narcotics |
| ICD-10-CM | T406a | Poisoning by and adverse effect of unspecified narcotics |
| Cocaine | ||
| ICD-10-CM | F141 | Cocaine abuse |
| ICD-10-CM | F142 | Cocaine dependence |
| ICD-10-CM | F149 | Cocaine use, unspecified |
| ICD-10-CM | T405a | Poisoning by and adverse effect of cocaine |
| Other stimulants | ||
| ICD-10-CM | F151 | Other stimulant abuse |
| ICD-10-CM | F152 | Other stimulant dependence |
| ICD-10-CM | F159 | Other stimulant use, unspecified |
| ICD-10-CM | T436a | Poisoning by and adverse effect of psychostimulants |
| All other substances | ||
| ICD-10-CM | F101 | Alcohol abuse |
| ICD-10-CM | F102 | Alcohol dependence |
| ICD-10-CM | F109 | Alcohol use, unspecified | ICD-10-CM | F121 | Cannabis abuse | ICD-10-CM | F122 | Cannabis dependence | ICD-10-CM | F129 | Cannabis use, unspecified | ICD-10-CM | F131 | Sedative, hypnotic or anxiolytic abuse | ICD-10-CM | F132 | Sedative, hypnotic or anxiolytic dependence | ICD-10-CM | F139 | Sedative, hypnotic or anxiolytic use, unspecified | ICD-10-CM | F161 | Hallucinogen abuse | ICD-10-CM | F162 | Hallucinogen dependence | ICD-10-CM | F169 | Hallucinogen use, unspecified | ICD-10-CM | F181 | Inhalant abuse | ICD-10-CM | F182 | Inhalant dependence | ICD-10-CM | F189 | Inhalant use, unspecified | ICD-10-CM | F191 | Other psychoactive substance abuse | ICD-10-CM | F192 | Other psychoactive substance dependence | ICD-10-CM | F199 | Other psychoactive substance use, unspecified | ICD-10-CM | G312 | Degeneration of nervous system due to alcohol | ICD-10-CM | G621 | Alcoholic polyneuropathy | ICD-10-CM | I426 | Alcoholic cardiomyopathy | ICD-10-CM | K292 | Alcoholic gastritis | ICD-10-CM | K70 | Alcoholic liver disease | ICD-10-CM | O354 | Maternal care for (suspected) damage to fetus from alcohol | ICD-10-CM | O355 | Maternal care for (suspected) damage to fetus by drugs | ICD-10-CM | O9931 | Alcohol use complicating pregnancy, childbirth, and the puerperium | ICD-10-CM | O9932 | Drug use complicating pregnancy, childbirth, and the puerperium | ICD-10-CM | T407a | Poisoning by and adverse effect of cannabis | ICD-10-CM | T408a | Poisoning by and adverse effect of lysergide (LSD) | ICD-10-CM | T4090a | Poisoning by and adverse effect of unspecified psychodysleptics (hallucinogens) | ICD-10-CM | T4099a | Poisoning by and adverse effect of other psychodysleptics (hallucinogens) | ICD-10-CM | T410X2a | Poisoning by and adverse effect of inhaled anesthetics, intentional self-harm |
| Preterm delivery | ||
| ICD-10-CM | O601 | Preterm labor with preterm delivery |
| ICD-10-CM | Z3A1-36 | Week of gestation <37 weeks |
| ICD-10-CM | O4201 | Preterm premature rupture of membranes, onset of labor within 24 hours of rupture |
| Severe pre-eclampsia and eclampsia | ||
| ICD-10-CM | O11 | Pre-existing hypertension with pre-eclampsia |
| ICD-10-CM | O141 | Severe pre-eclampsia |
| ICD-10-CM | O142 | HELLP syndrome |
| ICD-10-CM | O15 | Eclampsia |
| Placental abruption | ||
| ICD-10-CM | O45002 | Premature separation of placenta with coagulation defect, unspecified, second trimester |
| ICD-10-CM | O45003 | Premature separation of placenta with coagulation defect, unspecified, third trimester |
| ICD-10-CM | O45009 | Premature separation of placenta with coagulation defect, unspecified, unspecified trimester |
| ICD-10-CM | O45012 | Premature separation of placenta with afibrinogenemia, second trimester |
| ICD-10-CM | O45013 | Premature separation of placenta with afibrinogenemia, third trimester |
| ICD-10-CM | O45019 | Premature separation of placenta with afibrinogenemia, unspecified trimester |
| ICD-10-CM | O45022 | Premature separation of placenta with disseminated intravascular coagulation, second trimester |
| ICD-10-CM | O45023 | Premature separation of placenta with disseminated intravascular coagulation, third trimester |
| ICD-10-CM | O45029 | Premature separation of placenta with disseminated intravascular coagulation, unspecified trimester |
| ICD-10-CM | O45092 | Premature separation of placenta with other coagulation defect, second trimester |
| ICD-10-CM | O45093 | Premature separation of placenta with other coagulation defect, third trimester |
| ICD-10-CM | O45099 | Premature separation of placenta with other coagulation defect, unspecified trimester |
| ICD-10-CM | O458X2 | Other premature separation of placenta, second trimester |
| ICD-10-CM | O458X3 | Other premature separation of placenta, third trimester |
| ICD-10-CM | O458X9 | Other premature separation of placenta, unspecified trimester |
| ICD-10-CM | O4590 | Premature separation of placenta, unspecified, unspecified trimester |
| ICD-10-CM | O4592 | Premature separation of placenta, unspecified, second trimester |
| ICD-10-CM | O4593 | Premature separation of placenta, unspecified, third trimester |
| Obstetric hemorrhage/placenta accreta | ||
| ICD-10-CM | O43.212 | Placenta accreta, second trimester |
| ICD-10-CM | O43.213 | Placenta accreta, third trimester |
| ICD-10-CM | O43.219 | Placenta accreta, unspecified trimester |
| ICD-10-CM | O43.222 | Placenta increta, second trimester |
| ICD-10-CM | O43.223 | Placenta increta, third trimester |
| ICD-10-CM | O43.229 | Placenta increta, unspecified trimester |
| ICD-10-CM | O43.232 | Placenta percreta, second trimester |
| ICD-10-CM | O43.233 | Placenta percreta, third trimester |
| ICD-10-CM | O43.239 | Placenta percreta, unspecified trimester |
| ICD-10-CM | O72.0 | Third-stage hemorrhage |
| ICD-10-CM | O72.1 | Other immediate postpartum hemorrhage |
| ICD-10-CM | O72.2 | Delayed and secondary postpartum hemorrhage |
| ICD-10-CM | O72.3 | Postpartum coagulation defects |
| ICD-10-CM | O46.002 | Antepartum hemorrhage with coagulation defect, unspecified, second trimester |
| ICD-10-CM | O46.003 | Antepartum hemorrhage with coagulation defect, unspecified, third trimester |
| ICD-10-CM | O46.009 | Antepartum hemorrhage with coagulation defect, unspecified, unspecified trimester |
| ICD-10-CM | O46.012 | Antepartum hemorrhage with afibrinogenemia, second trimester |
| ICD-10-CM | O46.013 | Antepartum hemorrhage with afibrinogenemia, third trimester |
| ICD-10-CM | O46.019 | Antepartum hemorrhage with afibrinogenemia, unspecified trimester |
| ICD-10-CM | O46.022 | Antepartum hemorrhage with disseminated intravascular coagulation, second trimester |
| ICD-10-CM | O46.023 | Antepartum hemorrhage with disseminated intravascular coagulation, third trimester |
| ICD-10-CM | O46.029 | Antepartum hemorrhage with disseminated intravascular coagulation, unspecified trimester |
| ICD-10-CM | O46.092 | Antepartum hemorrhage with other coagulation defect, second trimester |
| ICD-10-CM | O46.093 | Antepartum hemorrhage with other coagulation defect, third trimester |
| ICD-10-CM | O46.099 | Antepartum hemorrhage with other coagulation defect, unspecified trimester |
| ICD-10-CM | O46.8X2 | Other antepartum hemorrhage, second trimester |
| ICD-10-CM | O46.8X3 | Other antepartum hemorrhage, third trimester |
| ICD-10-CM | O46.8X9 | Other antepartum hemorrhage, unspecified trimester |
| ICD-10-CM | O46.92 | Antepartum hemorrhage unspecified, second trimester |
| ICD-10-CM | O46.93 | Antepartum hemorrhage unspecified, third trimester |
| ICD-10-CM | O46.90 | Antepartum hemorrhage unspecified, unspecified trimester |
| Abbreviations: DRG, diagnosis-related group; HELLP, hemolysis, elevated liver enzymes, low platelet count; ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification; ICD-10-PCS, International Classification of Diseases, Tenth Revision, Procedure Coding System a Includes all codes in the series except for underdosing (sixth digit equal to 6) and sequela (seventh digit equal to S) | ||
Types of hospitals included in the HCUP National (Nationwide) Inpatient Sample The National (Nationwide) Inpatient Sample (NIS) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NIS includes obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Beginning in 2012, long-term acute care hospitals are also excluded. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay will be included in the NIS. Unit of analysis The unit of analysis is the hospital discharge (i.e., the hospital stay), not a person or patient. This means that a person who is admitted to the hospital for a delivery multiple times in 1 year will be counted each time as a separate discharge from the hospital. Location of patients' residence Place of residence is based on the urban-rural classification scheme for U.S. counties developed by the National Center for Health Statistics (NCHS). For this Statistical Brief, we collapsed the NCHS categories into either urban or rural according to the following: Urban:
The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska Department of Health and Social Services Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association Delaware Division of Public Health District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi State Department of Health Missouri Hospital Industry Data Institute Montana Hospital Association Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Department of Health and Human Resources, West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About the NIS The HCUP National (Nationwide) Inpatient Sample (NIS) is a nationwide database of hospital inpatient stays. The NIS is nationally representative of all community hospitals (i.e., short-term, non-Federal, nonrehabilitation hospitals). The NIS includes all payers. It is drawn from a sampling frame that contains hospitals comprising more than 95 percent of all discharges in the United States. The vast size of the NIS allows the study of topics at the national and regional levels for specific subgroups of patients. In addition, NIS data are standardized across years to facilitate ease of use. Over time, the sampling frame for the NIS has changed; thus, the number of States contributing to the NIS varies from year to year. The NIS is intended for national estimates only; no State-level estimates can be produced. The unweighted sample size for the 2016 NIS is 7,135,090 (weighted, this represents 35,675,421 inpatient stays). For More Information For other information on pregnancy and childbirth, including maternal hospital stays related to substance use, refer to the HCUP Statistical Briefs located at www.hcup-us.ahrq.gov/reports/statbriefs/sb_pregnancy.jsp. For additional HCUP statistics, visit:
For a detailed description of HCUP and more information on the design of the National Inpatient Sample (NIS), please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the National (Nationwide) Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated August 2018. www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed January 4, 2019. Suggested Citation Soni A (AHRQ), Fingar KR (IBM Watson Health), Reid LD (AHRQ). Obstetric Delivery Inpatient Stays Involving Substance Use Disorders and Related Clinical Outcomes, 2016. HCUP Statistical Brief #254. October 2019. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb254-Delivery-Hospitalizations-Substance-Use-Clinical-Outcomes-2016.pdf. Acknowledgments The authors would like to acknowledge the contributions of Marguerite Barrett of ML Barrett, Inc. and Minya Sheng of IBM Watson Health. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:Joel W. Cohen, Ph.D., Director Center for Financing, Access and Cost Trends Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 This Statistical Brief was posted online on October 29, 2019. 1 Ahrnsbrak R, Bose J, Hedden SL, Lipari RN, Park-Lee E. Key Substance Use and Mental Health Indicators in the United States: Results From the 2016 National Survey on Drug Use and Health. HHS Publication No. SMA 17-5044, NSDUH Series H-52. 2017. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. www.samhsa.gov/data/sites/default/files/NSDUH-FFR1-2016/NSDUH-FFR1-2016.htm. Accessed August 6, 2019. 2 Merikangas KR, McClair VL. Epidemiology of substance use disorders. Human Genetics. 2012;131(6):779-89. 3 McCance-Katz EF. The National Survey on Drug Use and Health: 2017. Substance Abuse and Mental Health Services Administration. www.samhsa.gov/data/sites/default/files/nsduh-ppt-09-2018.pdf. Accessed August 6, 2019. 4 Fingar KR, Stocks C, Weiss AJ, Owens PL. Neonatal and Maternal Hospital Stays Related to Substance Use, 2006-2012. HCUP Statistical Brief #193. July 2015. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb193-Neonatal-Maternal-Hospitalizations-Substance-Use.pdf. Accessed August 6, 2019. 5 Hudak ML, Tan RC. The Committee on Drugs and the Committee on Fetus and Newborn. Neonatal drug withdrawal. Pediatrics. 2012;129:e540. 6 Ibid. 7 Ibid. 8 Fingar KR et al., 2015. Op. cit. 9 National Institute on Drug Abuse. What are the effects of maternal cocaine use? www.drugabuse.gov/publications/research-reports/cocaine/what-are-effects-maternal-cocaine-use. Accessed August 6, 2019. 10 MacDorman MF, Declercq E, Cabral H, Morton C. Recent increases in the US maternal mortality rate: disentangling trends from measurement issues. Obstetrics & Gynecology, 2016;128(3):447-55. 11 Rural Health Information Hub. Substance abuse in rural areas. www.ruralhealthinfo.org/topics/substance-abuse. Accessed September 11, 2019. 12 Jumah, MA. Rural, Pregnant, and Opioid Dependent: A Systematic Review. Substance Abuse. 2016;10(Suppl 1):35-41. 13 García MC, Heilig CM, Lee SH, Faul M, Guy G, Iademarco MF, et al. Opioid prescribing rates in nonmetropolitan and metropolitan counties among primary care providers using an electronic health record system — United States, 2014-2017. Morbidity and Mortality Weekly Report. 2019;68:25-30. 14 Jumah, 2016. Op. cit. 15 Ibid. |
| Supplemental Table 1. Rates of delivery stays involving SUDs among patients residing in rural versus urban counties, overall and for select types of SUD diagnoses, 2016, for data presented in Figure 1 | ||||
| Rate per 1,000 delivery hospitalizations | Any SUD diagnosis | Opioids | Cocaine | Other stimulants |
|---|---|---|---|---|
| All locations (N=3,783,800 delivery stays) | 24.3 | 7.6 | 1.5 | 2.8 |
| Rural (N=507,700 delivery stays) | 35.7 | 11.6 | 1.3 | 4.9 |
| Urban (N=3,265,700 delivery stays) | 22.5 | 7.0 | 1.5 | 2.4 |
| Supplemental Table 2. Comparison of clinical outcomes among delivery stays with and without an SUD diagnosis, 2016, for data presented in Figure 2 | ||||||||||||
| Rate per 1,000 delivery hospitalizations | No SUD diagnosis | Any SUD diagnosis | Opioids | Cocaine | Other stimulants | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Preterm delivery | 98.9 | 206.8 | 229.1 | 349.3 | 295.9 | |||||||
| Severe pre-eclampsia/eclampsia | 28.9 | 41.9 | 38.4 | 58.7 | 80.1 | |||||||
| Obstetric hemorrhage/placenta accreta | 35.4 | 42.0 | 42.4 | 52.4 | 53.6 | |||||||
| Placental abruption | 10.2 | 33.7 | 36.8 | 69.3 | 60.2 | |||||||