STATISTICAL BRIEF #246 |
December 2018
William J. Freeman, Dr.PH., M.P.H., Audrey J. Weiss, Ph.D., and Kevin C. Heslin, Ph.D. Introduction Geographic differences in healthcare utilization and costs in the United States have been well documented.1 For example, in the last Healthcare Cost and Utilization Project (HCUP) Statistical Brief overviewing U.S. hospital stays in 2012, substantial differences were reported by census region.2 In particular, the West had the lowest rate of hospitalizations (97.2 per 1,000 population vs. over 120 per 1,000 population in other regions) but the highest average cost of hospital stays ($12,300 vs. less than $11,000 in other regions).3 In another study using 2016 data, the rate of hospital admissions ranged from 186 per 1,000 population in the District of Columbia to 69 per 1,000 population in Alaska.4 Factors such as differences in patient health status, treatment preferences, physician practice patterns, access to and availability of services, and wages/cost of living may help explain these types of geographic variation. This HCUP Statistical Brief presents statistics on hospital inpatient stays in 2016, with a focus on geographic variation based on the nine U.S. census divisions. The number and distribution of hospital stays are presented overall, along with the population rate, mean cost, and mean length of stay overall and by census division. For both the United States as a whole and for each census division, the rate of stays is presented by select patient characteristics (age, sex community-level income, and patient residence location) and the distribution of stays is provided by expected primary payer. Because of the large sample sizes, we focus on the size of differences between estimates rather than statistical significance. Findings Characteristics of hospital stays, 2016 Table 1 presents statistics on utilization and costs for hospital inpatient stays in 2016 by select patient characteristics. |
|
| Table 1. Number, percentage, and rate of hospital stays, length of stay, and costs by patient characteristics, 2016 | ||||||
| Characteristic | Hospital stays | Mean length of stay, days | Costs | |||
|---|---|---|---|---|---|---|
| Number, thousands | Percent | Rate per 1,000 population | Mean cost per stay, $ | Aggregate cost, millions $ | ||
| All hospital stays | 35,700 | 100.0 | 104.2 | 4.6 | 11,700 | 417,426 |
| Patient age, years | ||||||
| <1 | 4,200 | 11.8 | 210.8 | 3.9 | 5,900 | 24,535 |
| 1-17 | 1,300 | 3.6 | 17.1 | 4.2 | 12,500 | 15,759 |
| 18-44 | 8,700 | 24.4 | 75.4 | 3.8 | 8,600 | 74,527 |
| 45-64 | 8,800 | 24.6 | 104.3 | 5.1 | 14,500 | 127,082 |
| 65-84 | 9,900 | 27.7 | 232.5 | 5.2 | 14,500 | 143,373 |
| 85+ | 2,800 | 7.8 | 455.7 | 5.1 | 11,300 | 32,026 |
| Patient sex | ||||||
| Male | 15,400 | 43.1 | 91.3 | 5.0 | 13,300 | 204,908 |
| Female | 20,200 | 56.6 | 116.6 | 4.3 | 10,500 | 212,252 |
| Community-level income | ||||||
| Quartile 1 (lowest income) | 10,800 | 30.3 | 122.7 | 4.8 | 11,000 | 118,270 |
| Quartile 2 | 8,900 | 24.9 | 107.7 | 4.6 | 11,400 | 101,329 |
| Quartile 3 | 8,400 | 23.5 | 96.3 | 4.5 | 11,900 | 99,668 |
| Quartile 4 (highest income) | 7,000 | 19.6 | 82.5 | 4.5 | 12,900 | 90,075 |
| Patient residence | ||||||
| Large central metropolitan | 10,700 | 30.0 | 100.7 | 4.7 | 12,300 | 130,938 |
| Large fringe metropolitan | 8,500 | 23.8 | 100.6 | 4.6 | 11,800 | 100,262 |
| Medium metropolitan | 7,400 | 20.7 | 103.1 | 4.6 | 11,100 | 82,067 |
| Small metropolitan | 3,300 | 9.2 | 104.1 | 4.5 | 11,200 | 36,435 |
| Micropolitan | 3,200 | 9.0 | 111.8 | 4.5 | 11,300 | 36,875 |
| Noncore | 2,400 | 6.7 | 122.7 | 4.6 | 11,600 | 28,412 |
| Expected primary payer | ||||||
| Medicare | 14,100 | 39.5 | n/a | 5.3 | 13,600 | 192,784 |
| Medicaid | 8,200 | 23.0 | n/a | 4.6 | 9,800 | 81,153 |
| Private insurance | 10,700 | 30.0 | n/a | 3.9 | 10,900 | 115,852 |
| Uninsured | 1,500 | 4.2 | n/a | 4.1 | 9,300 | 13,781 |
| Other | 1,100 | 3.1 | n/a | 4.6 | 12,600 | 13,354 |
| Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2016 | ||||||
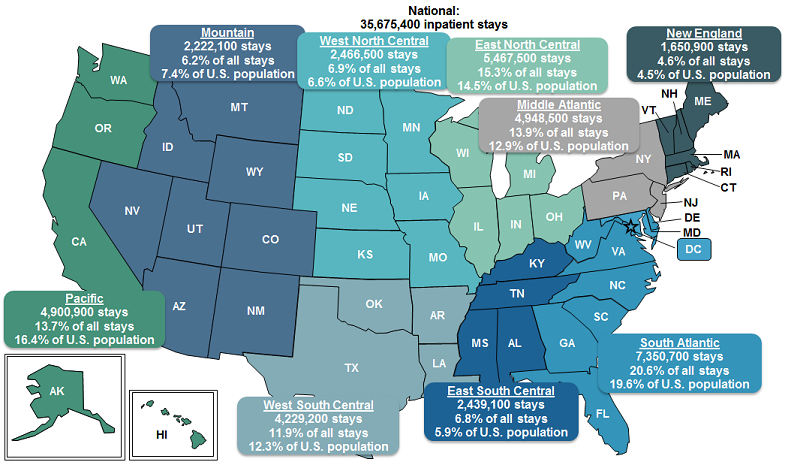
Figure 1 presents the total number and percentage of inpatient stays by U.S. census division in 2016. |
|
Figure 1. Number and percentage of inpatient stays by U.S. census division, 2016
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2016 Map of the United States that shows the number of inpatient stays, the percentage of inpatient stays, and the percentage of the U.S. population in each U.S. census division in 2016. National: 35,675,400 stays. Pacific: 4,900,900 stays, 13.7% of all stays, 16.4% of U.S. population. Mountain: 2,222,100 stays, 6.2% of all stays, 7.4% of U.S. population. West North Central: 2,466,500 stays, 6.9% of all stays, 6.6% of U.S. population. East North Central: 5,467,500 stays, 15.3% of all stays, 14.5% of U.S. population. Middle Atlantic: 4,948,500 stays, 13.9% of all stays, 12.9% of U.S. population. New England: 1,650,900 stays, 4.6% of all stays, 4.5% of U.S. population. South Atlantic: 7,350,700 stays, 20.6% of all stays, 19.6% of U.S. population. East South Central: 2,439,100 stays, 6.8% of all stays, 5.9% of U.S. population. West South Central: 4,229,200 stays, 11.9% of all stays, 12.3% of U.S. population.
|
|
|
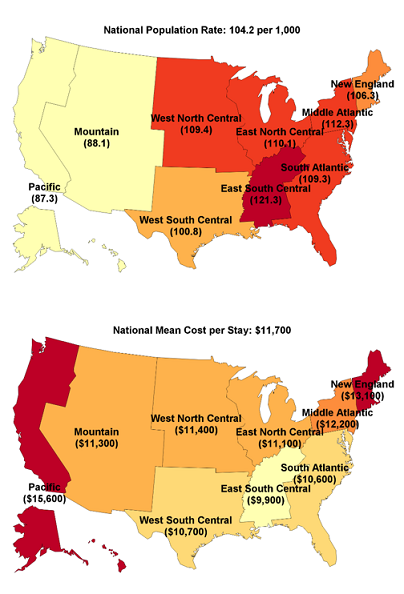
Figure 2. Population rate, mean cost, and mean length of stay of inpatient stays by U.S. census division, and ratio of census division rate to national rate, 2016 |
|
|
KEY FINDINGS BY MEASURE
KEY FINDINGS BY DIVISION
|
Table 2 presents the rate per 1,000 population of inpatient stays by patient age and sex by U.S. census division in 2016.
|
| Table 2. Population rate of inpatient stays by patient age and sex, by U.S. census division, 2016 | ||||||||||
| Variable | National | New England | Middle Atlantic | East North Central | West North Central | South Atlantic | East South Central | West South Central | Mountain | Pacific |
|---|---|---|---|---|---|---|---|---|---|---|
| Population rate per 1,000 | 104.2 | 106.3 | 112.3 | 110.1 | 109.4 | 109.3 | 121.3 | 100.8 | 88.1 | 87.3 |
| Patient age, years | ||||||||||
| <1 | 210.8 | 215.4 | 212.9 | 212.3 | 219.9 | 211.4 | 218.6 | 210.2 | 195.6 | 207.5 |
| 1-17 | 17.1 | 16.7 | 20.0 | 16.4 | 20.6 | 17.4 | 18.1 | 16.3 | 15.1 | 15.1 |
| 18-44 | 75.4 | 71.2 | 79.3 | 77.0 | 80.3 | 78.6 | 86.0 | 75.8 | 69.2 | 65.3 |
| 45-64 | 104.3 | 98.4 | 109.9 | 109.9 | 105.2 | 111.0 | 130.9 | 105.4 | 86.8 | 84.1 |
| 65-84 | 232.5 | 234.2 | 242.3 | 252.6 | 241.9 | 233.2 | 272.4 | 244.2 | 193.7 | 191.9 |
| 85+ | 455.7 | 488.3 | 483.3 | 477.6 | 445.4 | 454.1 | 500.9 | 481.5 | 362.5 | 406.1 |
| Patient sex | ||||||||||
| Male | 91.3 | 96.2 | 101.6 | 96.8 | 94.9 | 96.9 | 105.3 | 84.9 | 76.1 | 75.8 |
| Female | 116.6 | 115.9 | 122.5 | 122.9 | 123.5 | 121.0 | 136.5 | 116.3 | 100.1 | 98.7 |
| Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2016 | ||||||||||
|
|
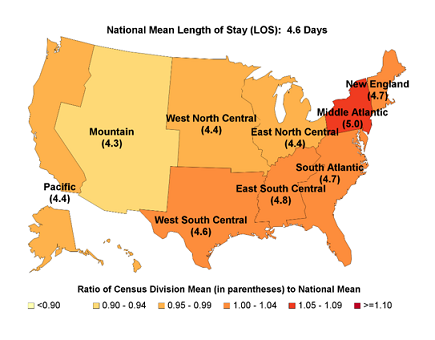
Figure 3. Population rate of inpatient stays by community-level income for each U.S. census division, 2016
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2016 Bar chart that shows the rate per 1,000 population of inpatient stays by community-level income by census division in 2016. National: Quartile 1 (lowest), 122.7; Quartiles 2-4 (higher incomes), 95.4. New England: Quartile 1 (lowest), 133.2; Quartiles 2-4 (higher incomes), 99.9. Middle Atlantic: Quartile 1 (lowest), 133.9; Quartiles 2-4 (higher incomes), 105.0. East North Central: Quartile 1 (lowest), 131.7; Quartiles 2-4 (higher incomes), 101.9. West North Central: Quartile 1 (lowest), 128.3; Quartiles 2-4 (higher incomes), 103.6. South Atlantic: Quartile 1 (lowest), 129.4; Quartiles 2-4 (higher incomes), 97.4. East South Central: Quartile 1 (lowest), 133.3; Quartiles 2-4 (higher incomes), 106.8. West South Central: Quartile 1 (lowest), 111.7; Quartiles 2-4 (higher incomes), 92.2. Mountain: Quartile 1 (lowest), 100.0; Quartiles 2-4 (higher incomes), 80.4. Pacific: Quartile 1 (lowest), 101.6; Quartiles 2-4 (higher incomes), 82.1.
|
|
|
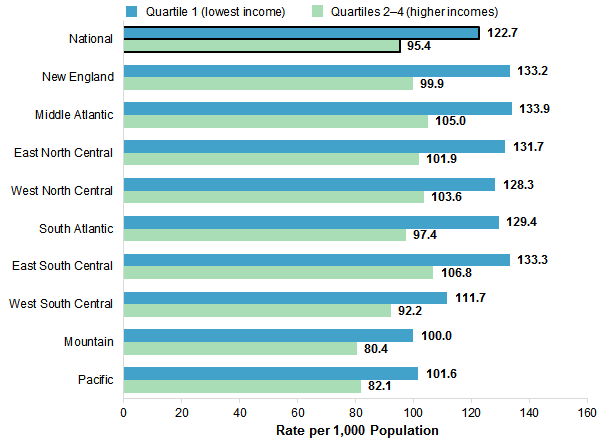
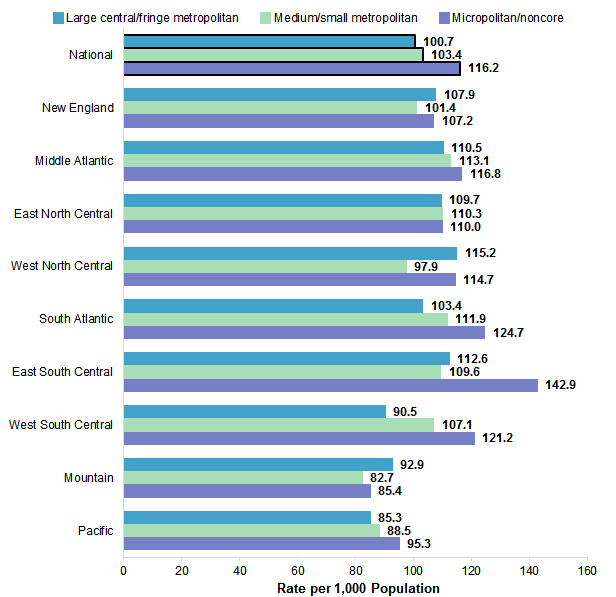
Figure 4. Population rate of inpatient stays by patient residence location for each U.S. census division, 2016
Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2016 Bar chart that shows the rate per 1,000 population of inpatient stays by patient residence location by U.S. census division in 2016. National: large central/fringe metropolitan, 100.7; medium/small metropolitan, 103.4; micropolitan/noncore, 116.2. New England: large central/fringe metropolitan, 107.9; medium/small metropolitan, 101.4; micropolitan/noncore, 107.2. Middle Atlantic: large central/fringe metropolitan, 110.5; medium/small metropolitan, 113.1; micropolitan/noncore, 116.8. East North Central: large central/fringe metropolitan, 109.7; medium/small metropolitan, 110.3; micropolitan/noncore, 110.0. West North Central: large central/fringe metropolitan, 115.2; medium/small metropolitan, 97.9; micropolitan/noncore, 114.7. South Atlantic: large central/fringe metropolitan, 103.4; medium/small metropolitan, 111.9; micropolitan/noncore, 124.7. East South Central: large central/fringe metropolitan, 112.6; medium/small metropolitan, 109.6; micropolitan/noncore, 142.9. West South Central: large central/fringe metropolitan, 90.5; medium/small metropolitan, 107.1; micropolitan/noncore, 121.2. Mountain: large central/fringe metropolitan, 92.9; medium/small metropolitan, 82.7; micropolitan/noncore, 85.4. Pacific: large central/fringe metropolitan, 85.3; medium/small metropolitan, 88.5; micropolitan/noncore, 95.3.
|
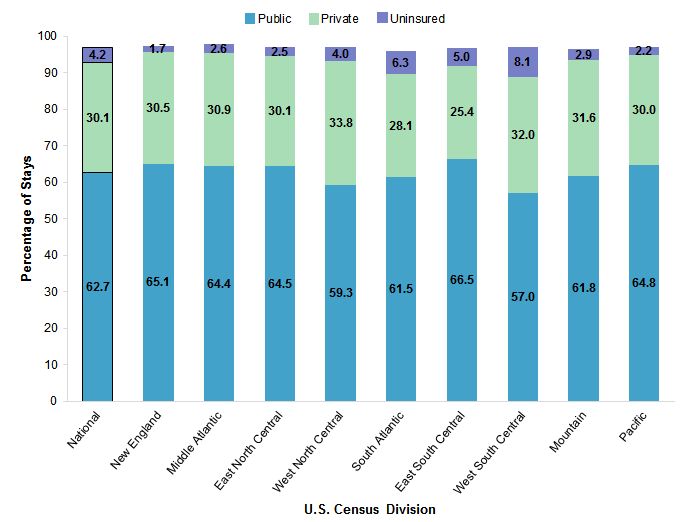
Figure 5 presents the percentage of inpatient stays by expected primary payer (public, private, and uninsured) for each U.S. census division in 2016. The distribution of stays for the different payer types by U.S. census division in 2016 is presented in the Appendix. |
|
Figure 5. Percentage of inpatient stays by expected primary payer for each U.S. census division, 2016
Note: Totals may not sum to 100 percent because of discharges with missing expected primary payer. Bar chart that shows the percentage of inpatient stays by expected primary payer by census division in 2016. National: public, 62.7; private, 30.1; uninsured, 4.2. New England: public, 65.1; private, 30.5; uninsured, 1.7. Middle Atlantic: public, 64.4; private, 30.9; uninsured, 2.6. East North Central: public, 64.5; private, 30.1; uninsured, 2.5. West North Central: public, 59.3; private, 33.8; uninsured, 4.0. South Atlantic: public, 61.5; private, 28.1; uninsured, 6.3. East South Central: public, 66.5; private, 25.4; uninsured, 5.0. West South Central: public, 57.0; private, 32.0; uninsured, 8.1. Mountain: public, 61.8; private, 31.6; uninsured, 2.9. Pacific: public, 64.8; private, 30.0; uninsured, 2.2.
|
Appendix. Population rate of inpatient stays by community-level income and patient residence, and percentage distribution of stays by primary payer, by U.S. census division, 2016
| Variable |
National |
New England |
Middle Atlantic |
East North Central |
West North Central |
South Atlantic |
East South Central |
West South Central |
Mountain |
Pacific |
Population rate per 1,000 |
104.2 |
106.3 |
112.3 |
110.1 |
109.4 |
109.3 |
121.3 |
100.8 |
88.1 |
87.3 |
Community-level income, rate |
Quartile 1 (lowest income) |
122.7 |
133.2 |
133.9 |
131.7 |
128.3 |
129.4 |
133.3 |
111.7 |
100.0 |
101.6 |
Quartile 2 |
107.7 |
119.0 |
114.1 |
112.8 |
114.1 |
111.4 |
121.3 |
104.8 |
86.7 |
93.2 |
Quartile 3 |
96.3 |
103.4 |
109.4 |
100.5 |
104.6 |
98.6 |
100.8 |
92.3 |
79.9 |
85.1 |
Quartile 4 (highest income) |
82.5 |
90.8 |
96.2 |
87.9 |
88.2 |
78.5 |
75.1 |
76.8 |
72.8 |
73.1 |
Patient residence location, rate |
Large central metropolitan |
100.7 |
112.1 |
112.6 |
116.4 |
117.8 |
111.8 |
104.6 |
89.9 |
95.1 |
85.8 |
Large fringe metropolitan |
100.6 |
106.0 |
108.4 |
102.7 |
113.6 |
98.3 |
122.3 |
91.8 |
86.2 |
83.6 |
Medium metropolitan |
103.1 |
98.2 |
112.3 |
111.9 |
99.0 |
111.1 |
122.1 |
104.9 |
80.1 |
86.6 |
Small metropolitan |
104.1 |
119.0 |
115.3 |
108.0 |
96.7 |
113.9 |
85.9 |
113.2 |
87.8 |
94.9 |
Micropolitan |
111.8 |
92.8 |
118.5 |
109.7 |
109.1 |
123.2 |
134.8 |
119.4 |
79.8 |
94.5 |
Noncore |
122.7 |
131.9 |
112.3 |
110.8 |
120.0 |
126.6 |
151.8 |
123.2 |
96.7 |
97.6 |
All hospital stays, N (millions) |
35.7 |
1.7 |
4.9 |
5.5 |
2.5 |
7.4 |
2.4 |
4.2 |
2.2 |
4.9 |
Primary payer, % |
Medicare |
39.6 |
44.2 |
40.1 |
42.8 |
41.2 |
41.0 |
43.7 |
35.7 |
34.8 |
34.4 |
Medicaid |
23.1 |
20.9 |
24.3 |
21.7 |
18.2 |
20.5 |
22.8 |
21.3 |
27.0 |
30.4 |
Private insurance |
30.1 |
30.5 |
30.9 |
30.1 |
33.8 |
28.1 |
25.4 |
32.0 |
31.6 |
30.0 |
Uninsured |
4.2 |
1.7 |
2.6 |
2.5 |
4.0 |
6.3 |
5.0 |
8.1 |
2.9 |
2.2 |
Other |
3.0 |
2.5 |
1.8 |
2.9 |
2.7 |
4.0 |
2.8 |
2.8 |
3.3 |
3.0 |
Note: Totals by primary payer may not sum to 100 percent due to discharges with missing payer information. | Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS), 2016 | ||||||||||||||||||||||||||||||||||||||||||||||||||