STATISTICAL BRIEF #244 |
September 2018
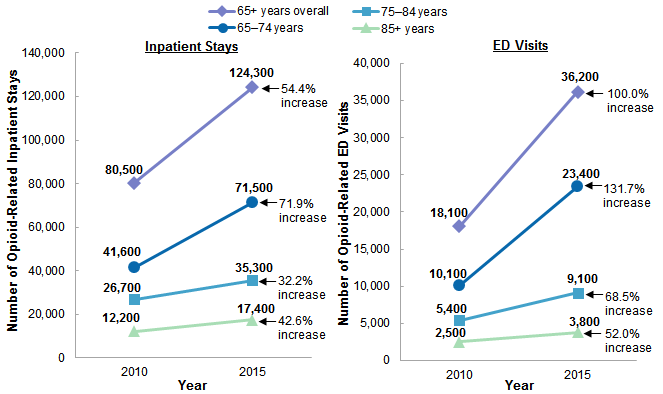
Audrey J. Weiss, Ph.D., Kevin C. Heslin, Ph.D., Marguerite L. Barrett, M.S., Rwaida Izar, M.P.H., and Arlene S. Bierman, M.D., M.S. Introduction Opioid misuse in older adults is an underappreciated and growing problem. Although opioid misuse overall is lower among older than among younger Americans, the rate of opioid misuse among older adults nearly doubled between 2002 and 2014.1 In 2016, a third of the more than 40 million Americans enrolled in Medicare Part D received prescription opioids and a substantial number received higher doses than recommended for prolonged periods of time, putting them at increased risk of misuse.2 Between 2005 and 2014, the rate of opioid-related hospitalizations increased fastest among patients aged 65 years and older compared with all other age groups.3 Eighty percent of U.S. adults aged 65 years and older have multiple chronic conditions (e.g., heart disease, diabetes, arthritis, and depression) compared with less than 20 percent of adults aged 18-44 years.4 Chronic pain is common among older adults,5 and more than one-third of older Americans are living with a disability,6 making this population more likely than younger adults to receive an opioid prescription.7 In addition, complex social needs and mental health issues including depression, substance abuse, cognitive decline, and dementia often go unrecognized and/or complicate clinical management.8, 9 Compounded by the physiologic changes associated with aging, these conditions place older adults using opioid medications at increased risk for adverse events including injurious falls10 and delirium,11 which may result in ED visits or hospital admissions. Additionally, older adults are more likely than younger adults to take prescription medications,12 which increases the likelihood of drug interactions and adverse effects associated with the use of opioids. In the period from 2011-2014, more than 90 percent of Americans aged 65 years and older reported use of a prescription drug in the past 30 days, with over 40 percent reporting use of five or more prescription drugs in the prior 30 days (compared with less than 5 percent of adults aged 18-44 years).13 This represents a substantial increase in the proportion of adults aged 65 years and older who used prescription medications compared with 20 years earlier (1988-1994: one prescription medication, 74 percent; five or more prescription medications, 14 percent).14 This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents statistics on opioid-related hospital stays and ED visits among patients aged 65 years and older in fiscal year (FY) 2010 (from quarter 4 of 2009 through quarter 3 of 2010) and FY 2015 (from quarter 4 of 2014 through quarter 3 of 2015), hereinafter referred to as 2010 and 2015.15 The number and rate of opioid-related stays and ED visits in 2010 and 2015 are provided for three distinct age groups: 65-74 years, 75-84 years, and 85 years and older. The percentage of opioid-related inpatient stays and ED visits that involved a principal opioid diagnosis is provided for each of the three age groups in 2015. Characteristics of opioid-related stays and ED visits versus nonopioid-related stays and visits among adults aged 65 years and older are presented for 2015. Identification of opioid-related stays and ED visits is based on all-listed diagnoses and includes events associated with prescription opioids or illicit opioids such as heroin. Differences greater than 10 percent between estimates are noted in the text. Findings Distribution of opioid-related inpatient stays and ED visits among patients aged 65 years and older, 2010 and 2015 Figure 1 provides the number of opioid-related inpatient stays and ED visits among patients aged 65 years and older by patient age group in 2010 and 2015. |
|
|
Figure 1. Number of opioid-related inpatient stays and ED visits among patients aged 65 years and older, by age group, 2010 versus 2015
Abbreviation: ED, emergency department Two line graphs, one for inpatient stays and one for ED visits, that show the number of opioid-related inpatient stays or ED visits among patients aged 65+ years by age group in 2010 and 2015. Inpatient stays: 65+ years: 2010, 80,500; 2015, 124,300, for a 54.4% cumulative increase. 65-74 years: 2010, 41,600; 2015, 71,500, for a 71.9% increase. 75-84 years: 2010, 26,700; 2015, 35,300, for a 32.2% increase. 85+ years: 2010, 12,200; 2015, 17,400, for a 42.6% cumulative increase. ED visits: 65+ years: 2010, 18,100; 2015, 36,200, for a 100.0% cumulative increase. 65-74 years: 2010, 10,100; 2015, 23,400, for a 131.7% increase. 75-84 years: 2010, 5,400; 2015, 9,100, for a 68.5% increase. 85+ years: 2010, 2,500; 2015, 3,800, for a 52.0% cumulative increase. |
|
|
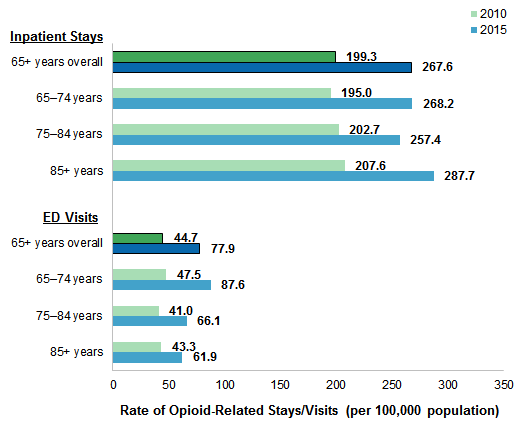
Figure 2. Population rate of opioid-related inpatient stays and ED visits among patients aged 65 years and older, by age group, 2010 versus 2015
Abbreviation: ED, emergency department Two bar charts, one for inpatient stays and one for ED visits, that show the rate of opioid-related inpatient stays and ED visits per 100,000 population among patients aged 65+ years by age group in 2010 and 2015. Inpatient stays: 65+ years: 2010, 199.3; 2015, 267.6. 65-74 years: 2010, 195.0; 2015, 268.2. 75-84 years: 2010, 202.7; 2015, 257.4. 85+ years: 2010, 207.6; 2015, 287.7. ED visits: 65+ years: 2010, 44.7; 2015, 77.9. 65-74 years: 2010, 47.5; 2015, 87.6. 75-84 years: 2010, 41.0; 2015, 66.1. 85+ years: 2010, 43.3; 2015, 61.9. |
|
|
Figure 3. Change in the rate of opioid-related inpatient stays and ED visits among patients aged 65 years and older, by age group, 2010 versus 2015
Abbreviation: ED, emergency department Two bar charts, one for inpatient stays and one for ED visits, that show the percentage change in rate of opioid-related stays and visits among patients aged 65+ years by age group in 2010 and 2015. Inpatient stays: 65+ years overall, 34.3; 65-74 years, 37.6; 75-84 years, 27.0; 85+ years, 38.6, compared with minus 17.4 for non-opioid-related stays. ED visits: 65+ years overall, 74.2; 65-74 years, 84.5; 75-84 years, 61.5; 85+ years, 43.2, compared with 17.4 for non-opioid-related stays. |
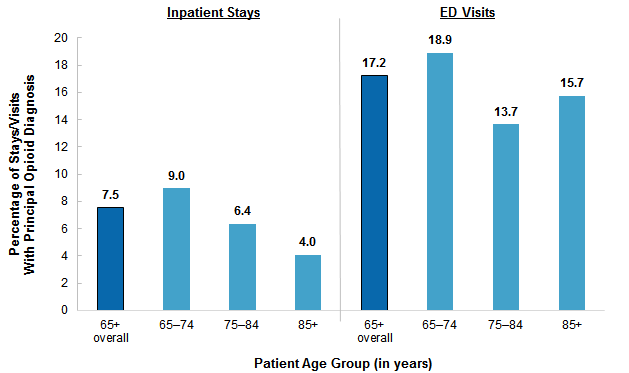
Figure 4 presents the percentage of opioid-related inpatient stays and ED visits that involved a principal opioid diagnosis among patients aged 65 years and older, by patient age group, in 2015. |
|
Figure 4. Principal opioid diagnosis among opioid-related inpatient stays and ED visits for patients aged 65 years and older, by age group, 2015
Abbreviation: ED, emergency department Two bar charts, one for inpatient stays and one for ED visits, that show the percentage of opioid-related stays and visits with a principal opioid diagnosis by age group in 2015. Inpatient stays: 65+ overall, 7.5; 65-74 years, 9.0; 75-84 years, 6.4; 85+ years, 4.0. ED visits: 65+ overall, 17.2; 65-74 years, 18.9; 75-84 years, 13.7; 85+ years, 15.7. |
|
| Table 1. Resource use for opioid-related versus nonopioid-related inpatient stays and ED visits among patients aged 65 years and older, 2015 | |||
| Variable | Opioid-related stays/visits | Nonopioid-related stays/visits | % difference |
|---|---|---|---|
| Number of inpatient stays | 124,300 | 12,537,100 | |
| Utilization characteristics | |||
| Average cost per stay, $ | 14,900 | 13,200 | 12.9 |
| Average length of stays, days | 6.0 | 5.2 | 14.4 |
| Discharge disposition, % | |||
| Routine discharge | 36.1 | 43.8 | -17.7 |
| Another short-term hospital | 1.9 | 2.4 | -22.5 |
| Another institution (SNF, ICF, etc.) | 36.9 | 29.6 | 24.4 |
| Home healthcare | 21.0 | 19.8 | 6.3 |
| Against medical advice | 1.4 | 0.5 | 165.6 |
| In-hospital death | 2.7 | 3.7 | -28.8 |
| Number of ED visits | 36,200 | 17,617,300 | |
| Utilization characteristics | |||
| Average charge per visit, $ | 6,600 | 4,900 | 34.7 |
| Discharge disposition, % | |||
| Routine discharge | 81.6 | 83.4 | -2.2 |
| Another short-term hospital | 2.5 | 4.1 | -40.1 |
| Another institution (SNF, ICF, etc.) | 6.2 | 3.7 | 66.7 |
| Home healthcare | 3.2 | 0.9 | 280.1 |
| Against medical advice | 1.6 | 1.1 | 38.5 |
| Died in ED | 0.3 | 0.6 | -56.4 |
| Abbreviation: ED, emergency department; ICF, intermediate care facility; SNF, skilled nursing facility Note: Number of stays/visits and average costs/charges were rounded to the nearest hundred. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), 2015 fiscal year data from the National (Nationwide) Inpatient Sample (NIS), 2014-2015; Nationwide Emergency Department Sample (NEDS), 2014-2015 | |||
|
|
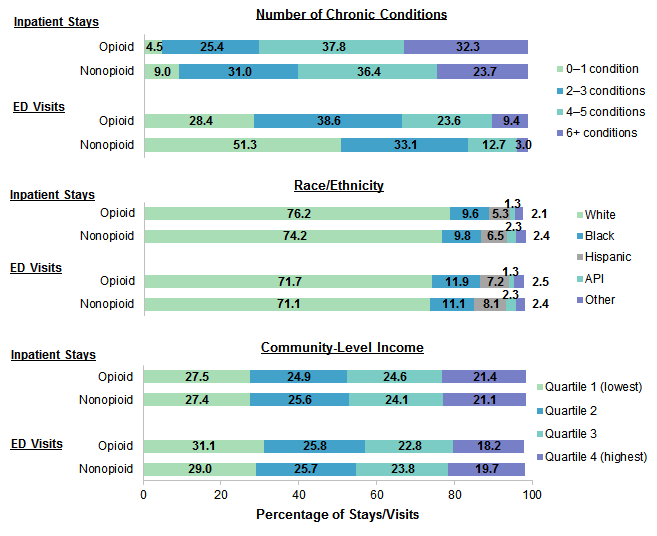
Figure 5. Opioid-related versus nonopioid-related inpatient stays and ED visits by number of chronic conditions, race/ethnicity, and community-level income among patients aged 65 years and older, 2015
Abbreviations: API, Asian/Pacific Islander; ED, emergency department Three bar charts—one for number of chronic conditions, one for race/ethnicity, and one for community-level income—that show these percentage distributions among opioid-related and non-opioid-related stays and visits for patients aged 65+ years in 2015. Number of chronic conditions: opioid inpatient stays: 0-1 condition, 4.5; 2-3 conditions, 25.4; 4-5 conditions, 37.8; 6+ conditions, 32.3. Nonopioid inpatient stays: 0-1 condition, 9.0; 2-3 conditions, 31.0; 4-5 conditions, 36.4; 6+ conditions, 23.7. Opioid ED visits: 0-1 condition, 28.4; 2-3 conditions, 38.6; 4-5 conditions, 23.6; 6+ conditions, 9.4. Nonopioid ED visits: 0-1 condition, 51.3; 2-3 conditions, 33.1; 4-5 conditions, 12.7; 6+ conditions, 3.0. Race/ethnicity: opioid inpatient stays: White, 76.2; Black, 9.6; Hispanic, 5.3; API, 1.3; Other, 2.1. Nonopioid inpatient stays: White, 74.2; Black, 9.8; Hispanic, 6.5; API, 2.3; Other, 2.4. Opioid ED visits: White, 71.7; Black, 11.9; Hispanic, 7.2; API, 1.3; Other, 2.5. Nonopioid ED visits: White, 71.1; Black, 11.1; Hispanic, 8.1; API, 2.3; Other, 2.4. Community-level income: opioid inpatient stays: Quartile 1 (lowest), 27.5; Quartile 2, 24.9; Quartile 3, 24.6; Quartile 4 (highest), 21.4. Nonopioid inpatient stays: Quartile 1 (lowest), 27.4; Quartile 2, 25.6; Quartile 3, 24.1; Quartile 4 (highest), 21.1. Opioid ED visits: Quartile 1 (lowest), 31.1; Quartile 2, 25.8; Quartile 3, 22.8; Quartile 4 (highest), 18.2. Nonopioid ED visits: Quartile 1 (lowest), 29.0; Quartile 2, 25.7; Quartile 3, 23.8; Quartile 4 (highest), 19.7. |
|
|
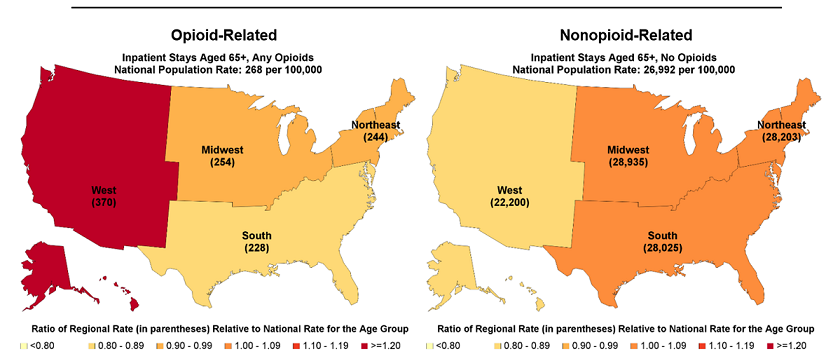
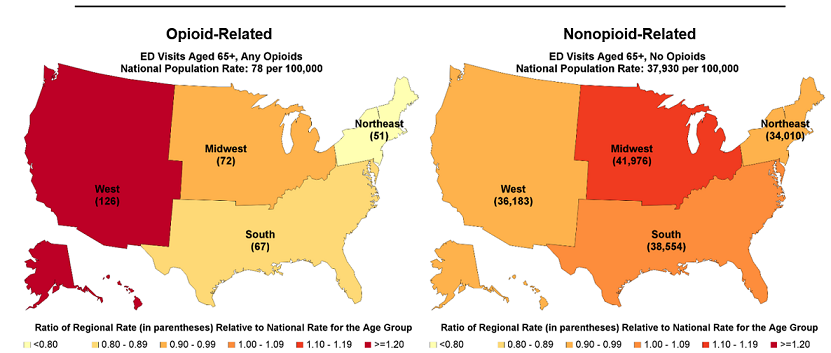
Figure 6. Rate of opioid-related versus nonopioid-related inpatient stays and ED visits among patients aged 65 years and older by census region, and ratio of census region to national rate, 2015
ED Visits
Abbreviation: ED, emergency department Four colored maps that show the rate per 100,000 population of opioid- and non-opioid-related inpatient stays and ED visits among patients aged 65+ years by census region and ratio of census region to national rate in 2015. Opioid-related inpatient stays: national rate = 268; West, rate = 370, ratio to national rate >1.2; Midwest, rate = 254, ratio to national rate 0.90-0.99; South, rate = 228, ratio to national rate 0.80-0.89; Northeast, 244, ratio to national rate 0.90-0.99. Non-opioid-related inpatient stays: national rate = 26,992; West, rate = 22,200, ratio to national rate 0.80-0.89; Midwest, rate = 28,935, ratio to national rate 1.00-1.09; South, rate = 28,025, ratio to national rate 1.00-1.09; Northeast, 28,203, ratio to national rate 1.00-1.09. Opioid-related ED visits: national rate = 78; West, rate = 126, ratio to national rate <1.2; Midwest, rate = 72, ratio to national rate 0.90-0.99; South, rate = 67, ratio to national rate 0.80-0.89; Northeast, 51, ratio to national rate <0.80. Non-opioid-related ED visits: national rate = 37.930; West, rate = 36,183, ratio to national rate 0.90-0.99; Midwest, rate = 41,976, ratio to national rate 1.10-1.19; South, rate = 38,554, ratio to national rate 1.00-1.09; Northeast, 34,010, ratio to national rate 0.90-0.99. |
Healthcare Cost and Utilization Project (HCUP) Statistical Briefs provide basic descriptive statistics on a variety of topics using HCUP administrative healthcare data. Topics include hospital inpatient, ambulatory surgery, and emergency department use and costs, quality of care, access to care, medical conditions, procedures, and patient populations, among other topics. The reports are intended to generate hypotheses that can be further explored in other research; the reports are not designed to answer in-depth research questions using multivariate methods. Data Source The estimates in this Statistical Brief are based upon data from the HCUP 2014-2015 National Inpatient Sample (NIS) and 2014-2015 Nationwide Emergency Department Sample (NEDS). Historical data were drawn from the 2009-2010 Nationwide Inpatient Sample (NIS) and 2009-2010 NEDS. In both sets of years, the calendar year databases were used to create a fiscal year file from October to September. The NEDS was limited to emergency department (ED) visits that do not result in an admission to the same hospital (i.e., ED admissions). ED admissions are included under inpatient stays. Supplemental sources included population denominator data for use with HCUP databases, derived from information available from Claritas, a vendor that compiles and adds value to data from the U.S. Census Bureau.16 Definitions Diagnoses, ICD-9-CM, and Clinical Classifications Software The principal diagnosis is that condition established after study to be chiefly responsible for the patient's admission to the hospital. Secondary diagnoses are concomitant conditions that coexist at the time of admission or develop during the stay. All-listed diagnoses include the principal diagnosis plus these additional secondary conditions. ICD-9-CM is the International Classification of Diseases, Ninth Revision, Clinical Modification, which assigns numeric codes to diagnoses. There are approximately 14,000 ICD-9-CM diagnosis codes. CCS categorizes ICD-9-CM diagnosis codes into a manageable number of clinically meaningful categories.17 This clinical grouper makes it easier to quickly understand patterns of diagnoses. CCS categories identified as Other typically are not reported; these categories include miscellaneous, otherwise unclassifiable diagnoses that may be difficult to interpret as a group. Case definition Opioid-related hospital use was identified using the following all-listed ICD-9-CM diagnosis codes:
These codes include opioid-related use stemming from illicit opioids such as heroin, illegal use of prescription opioids, and the use of opioids as prescribed. Each type of opioid use is important for understanding and addressing the opioid epidemic in the United States.18 Although there may be interest in examining how much each type of opioid use contributes to the overall opioid problem, many of the opioid-related codes under the ICD-9-CM clinical coding system do not allow heroin-related cases to be explicitly identified (e.g., in the 304.0x series, heroin is not distinguished from other opioids). In addition, the codes do not distinguish between illegal use of prescription drugs and their use as prescribed. Chronic conditions were identified using the set of chronic conditions developed by the U.S. Department of Health and Human Services (HHS) Interagency Workgroup on multiple chronic conditions (MCC) and the Office of the Assistant Secretary of Health.19 As reported by Goodman and colleagues (2013), 20 chronic conditions were identified with definitions for five selected HHS health data systems, including the HCUP Nationwide Inpatient Sample (NIS). For the HCUP inpatient databases, the 20 chronic conditions were defined using the Agency for Healthcare Research and Quality (AHRQ) Clinical Classifications Software (CCS), which groups together highly related diagnoses of the same condition. One condition, autism spectrum disorder, was defined using ICD-9-CM diagnosis codes rather than CCS categories. Steiner and Friedman (2013) implemented these chronic condition definitions in an analysis of MCC using the 2009 NIS.20 The 20 chronic conditions and corresponding clinical coding criteria are provided in Table 2. Consistent with Steiner and Friedman (2013), we identified chronic conditions on the basis of the clinical coding criteria (listed in Table 2) indicated in either a principal or a secondary diagnosis code field on the discharge record. A chronic condition was counted only once per discharge regardless of the number of diagnosis codes (principal and secondary) that indicated the condition. |
| Table 2. Chronic conditions and clinical coding criteria | |
| Chronic condition | Clinical coding criteria |
|---|---|
| Hypertension | CCS 98, 99 |
| Hyperlipidemia | CCS 53 |
| Congestive heart failure | CCS 108 |
| Coronary artery disease (CAD) (includes acute myocardial infarction, which indicates chronic underlying CAD) | CCS 100, 101 |
| Diabetes | CCS 49, 50 |
| Stroke (includes acute stroke but indicates underlying cerebrovascular disease) | CCS 109-112 |
| Cardiac arrhythmias | CCS 105, 106 |
| Arthritis | CCS 202, 203 |
| Cancer | CCS 11-43 |
| Depression | CCS 657 |
| Dementia (includes Alzheimer's and other senile dementias) | CCS 653 |
| Substance abuse disorders | CCS 660, 661 |
| Chronic obstructive pulmonary disease | CCS 127 |
| Asthma | CCS 128 |
| Chronic kidney disease | CCS 156, 158 |
| Human immunodeficiency virus (HIV) | CCS 5 |
| Hepatitis | CCS 6 |
| Autism spectrum disorder | ICD-9-CM 29900, 29901 |
| Schizophrenia | CCS 659 |
| Osteoporosis | CCS 206 |
| Abbreviations: CCS, Clinical Classifications Software; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification | |
Because the number of secondary diagnoses reported on hospital discharge and ED visit records in HCUP data has increased over time, we held the number of secondary diagnosis fields constant across both data years to ensure comparability: 25 diagnosis codes for hospital discharge records and 15 diagnosis codes for ED visit records.
Types of hospitals included in the HCUP National (Nationwide) Inpatient Sample The National (Nationwide) Inpatient Sample (NIS) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NIS includes obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Beginning in 2012, long-term acute care hospitals are also excluded. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay will be included in the NIS. Types of hospitals included in the HCUP Nationwide Emergency Department Sample The Nationwide Emergency Department Sample (NEDS) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NEDS includes specialty, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Hospitals included in the NEDS have hospital-owned EDs and no more than 90 percent of their ED visits resulting in admission. Unit of analysis The unit of analysis is the hospital discharge (i.e., the hospital stay) or the ED visit, not a person or patient. This means that a person who is admitted to the hospital or seen in the ED multiple times in 1 year will be counted each time as a separate discharge from the hospital or visit in the ED. Charges Charges represent what the hospital billed for the discharge. Hospital charges reflect the amount the hospital charged for the entire hospital stay and do not include professional (physician) fees. For the purposes of this Statistical Brief, charges are rounded to the nearest hundred dollars. Costs and charges Total hospital charges were converted to costs using HCUP Cost-to-Charge Ratios based on hospital accounting reports from the Centers for Medicare & Medicaid Services.21 Costs reflect the actual expenses incurred in the production of hospital services, such as wages, supplies, and utility costs; charges represent the amount a hospital billed for the case. For each hospital, a hospital-wide cost-to-charge ratio is used. Hospital charges reflect the amount the hospital billed for the entire hospital stay and do not include professional (physician) fees. For the purposes of this Statistical Brief, costs are reported to the nearest hundred. Annual costs were inflation adjusted using the Gross Domestic Product Price Index from the U.S. Department of Commerce, Bureau of Economic Analysis, with 2015 as the index base.22 That is, all costs are expressed in 2015 dollars. Annual charges were inflation adjusted using the Consumer Price Index for Urban Consumers from the U.S. Department of Labor, Bureau of Labor Statistics, with 2015 as the index base.23 That is, all charges are expressed in 2015 dollars. Community-level income Community-level income is based on the median household income of the patient's ZIP Code of residence. Quartiles are defined so that the total U.S. population is evenly distributed. Cut-offs for the quartiles are determined annually using ZIP Code demographic data obtained from Claritas, a vendor that adds value to data from the U.S. Census Bureau.24 The value ranges for the income quartiles vary by year. The income quartile is missing for patients who are homeless or foreign. Region Region is one of the four regions defined by the U.S. Census Bureau:
Discharge status reflects the disposition of the patient at discharge from the hospital and includes the following six categories: routine (to home), transfer to another short-term hospital, other transfers (including skilled nursing facility, intermediate care, and another type of facility such as a nursing home), home healthcare, against medical advice, or died in the hospital. Reporting of race and ethnicity Data on Hispanic ethnicity are collected differently among the States and also can differ from the census methodology of collecting information on race (White, Black, Asian/Pacific Islander, American Indian/Alaska Native, Other [including mixed race]) separately from ethnicity (Hispanic, non-Hispanic). State data organizations often collect Hispanic ethnicity as one of several categories that include race. Therefore, for multistate analyses, HCUP creates the combined categorization of race and ethnicity for data from States that report ethnicity separately. When a State data organization collects Hispanic ethnicity separately from race, HCUP uses Hispanic ethnicity to override any other race category to create a Hispanic category for the uniformly coded race/ethnicity data element, while also retaining the original race and ethnicity data. This Statistical Brief reports race/ethnicity for the following categories: Hispanic, non-Hispanic White, non-Hispanic Black, Asian/Pacific Islander, and non-Hispanic Other. About HCUP The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska Department of Health and Social Services Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association Delaware Division of Public Health District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi State Department of Health Missouri Hospital Industry Data Institute Montana Hospital Association Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Department of Health and Human Resources, West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About the NIS The HCUP National (Nationwide) Inpatient Sample (NIS) is a nationwide database of hospital inpatient stays. The NIS is nationally representative of all community hospitals (i.e., short-term, non-Federal, nonrehabilitation hospitals). The NIS includes all payers. It is drawn from a sampling frame that contains hospitals comprising more than 95 percent of all discharges in the United States. The vast size of the NIS allows the study of topics at the national and regional levels for specific subgroups of patients. In addition, NIS data are standardized across years to facilitate ease of use. Over time, the sampling frame for the NIS has changed; thus, the number of States contributing to the NIS varies from year to year. The NIS is intended for national estimates only; no State-level estimates can be produced. The 2012 NIS was redesigned to optimize national estimates. The redesign incorporates two critical changes:
About the NEDS The HCUP Nationwide Emergency Department Database (NEDS) is a unique and powerful database that yields national estimates of emergency department (ED) visits. The NEDS was constructed using records from both the HCUP State Emergency Department Databases (SEDD) and the State Inpatient Databases (SID). The SEDD capture information on ED visits that do not result in an admission (i.e., patients who were treated in the ED and then released from the ED, or patients who were transferred to another hospital); the SID contain information on patients initially seen in the ED and then admitted to the same hospital. The NEDS was created to enable analyses of ED utilization patterns and support public health professionals, administrators, policymakers, and clinicians in their decision making regarding this critical source of care. The NEDS is produced annually beginning in 2006. Over time, the sampling frame for the NEDS has changed; thus, the number of States contributing to the NEDS varies from year to year. The NEDS is intended for national estimates only; no State-level estimates can be produced. For More Information For other information on mental health and substance abuse, including opioids, refer to the HCUP Statistical Briefs located at www.hcup-us.ahrq.gov/reports/statbriefs/sb_mhsa.jsp. For additional HCUP statistics, visit:
For a detailed description of HCUP and more information on the design of the National (Nationwide) Inpatient Sample (NIS) and the National Emergency Department Sample (NEDS), please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the National (Nationwide) Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated February 2018. www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed February 12, 2018. Agency for Healthcare Research and Quality. Overview of the Nationwide Emergency Department Sample (NEDS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated December 2017. www.hcup-us.ahrq.gov/nedsoverview.jsp. Accessed January 18, 2018. Suggested Citation Fingar KR (IBM Watson Health), Skinner H (IBM Watson Health), Johann J (IBM Watson Health), Coenen N (IBM Watson Health), Freeman WJ (AHRQ), Heslin KC (AHRQ). Geographic Variation in Substance-Related Inpatient Stays Across States and Counties in the United States, 2013–2015. HCUP Statistical Brief #245. November 2018. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb244-Opioid-Inpatient-Stays-ED-Visits-Older-Adults.pdf. Acknowledgments The authors would like to acknowledge the contributions of Minya Sheng of IBM Watson Health. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:Virginia Mackay-Smith, Acting Director Center for Delivery, Organization, and Markets Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 This Statistical Brief was posted online on September 18, 2018. 1 Substance Abuse and Mental Health Services Administration. Opioid Misuse Increases Among Older Adults. National Survey on Drug Use and Health: The CBHSQ Report. July 25, 2017. www.samhsa.gov/data/sites/default/files/report_3186/Spotlight-3186.html. Accessed July 24, 2018. 2 U.S. Department of Health & Human Services, Office of Inspector General. Opioids in Medicare Part D: Concerns About Extreme Use and Questionable Prescribing. HHS OIG Data Brief. July 2017. www.oig.hhs.gov/oei/reports/oei-02-17-00250.pdf. Accessed July 24, 2018. 3 Weiss AJ, Bailey MK, O'Malley L, Barrett ML, Elixhauser A, Steiner CA. Patient Characteristics of Opioid-Related Inpatient Stays and Emergency Department Visits Nationally and by State, 2014. HCUP Statistical Brief #224. June 2017. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb224-Patient-Characteristics-Opioid-Hospital-Stays-ED-Visits-by-State.pdf. Accessed July 24, 2018. 4 Gerteis J, Izrael D, Deitz D, LeRoy L, Ricciardi R, Miller T, et al. Multiple Chronic Conditions Chartbook: 2010 Medical Expenditure Panel Survey Data. Rockville, MD: Agency for Healthcare Research and Quality; 2014. www.ahrq.gov/sites/default/files/wysiwyg/professionals/prevention-chronic-care/decision/mcc/mccchartbook.pdf. Accessed July 27, 2018. 5 Institute of Medicine, Board on Health Sciences Policy, Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: The National Academies Press; 2011. 6 He W, Larsen LJ. Older Americans With a Disability: 2008-2012. U.S. Census Bureau, American Community Survey Reports, ACS-29. U.S. Government Printing Office, Washington, DC; 2014. 7 Centers for Disease Control and Prevention. Annual Surveillance Report of Drug-Related Risks and Outcomes—United States, 2017. Surveillance Special Report 1. Centers for Disease Control and Prevention. August 31, 2017. www.cdc.gov/drugoverdose/pdf/pubs/2017-cdc-drug-surveillance-report.pdf. Accessed July 27, 2018. 8 Bartels SJ, Blow FC, Brockmann LM, Van Citters AD. Substance Abuse and Mental Health Among Older Americans: The State of the Knowledge and Future Directions. Report prepared for the Substance Abuse and Mental Health Services Administration. Rockville MD: Westat; 2005. www.gsa-alcohol.fmhi.usf.edu/Substance%20Abuse%20and%20Mental%20Health%20Among%20Older%20Adults-%20The%20State%20of%20Knowledge%20and%20Future%20Directions.pdf. Accessed August 6, 2018. 9 Valtorta N, Hanratty B. Loneliness, isolation and the health of older adults: do we need a new research agenda? Journal of the Royal Society of Medicine. 2012 Dec;105(12):518-22. 10 Miller M, Sturmer T, Azrael D, Levin R, Solomon DH. Opioid analgesics and the risk of fractures among older adults with arthritis. Journal of the American Geriatrics Society. 2011;59(3):430-8. 11 Pisani MA, Murphy TE, Araujo KLB, Van Ness PH. Factors associated with persistent delirium following ICU admission in an older medical patient population. Journal of Critical Care. 2010;25(3):540.e1-540.e7. 12 National Center for Health Statistics. Health, United States, 2016: With Chartbook on Long-Term Trends in Health. Table 79. Hyattsville, MD: National Center for Health Statistics; 2017. www.cdc.gov/nchs/data/hus/hus16.pdf. Accessed July 30, 2018. 13 Ibid. 14 Ibid. 15 We used fiscal years (FYs) in this Statistical Brief because beginning FY 2016, on October 1, 2015, the United States transitioned from the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) clinical coding system to the International Classification of Diseases, Tenth Revision, Clinical Modification/Procedural Coding System (ICD-10-CM/PCS) clinical coding system. Although codes for opioid-related diagnoses are available in both coding systems, the change in coding systems resulted in a substantial shift in the number of opioid-related inpatient stays (ref. Heslin KC, Owens PL, Karaca Z, Barrett ML, Moore BJ, Elixhauser A. Trends in opioid-related inpatient stays shifted after the US transitioned to ICD-10-CM diagnosis coding in 2015. Medical Care. 2017;55(11):918-23). As a result, for comparability across years in this Statistical Brief, we used 2 FYs (2010 and 2015) with clinical coding entirely under the ICD-9-CM coding system. 16 Claritas. Claritas Demographic Profile. www.claritas.com. 17 Agency for Healthcare Research and Quality. HCUP Clinical Classifications Software (CCS) for ICD-9-CM. Healthcare Cost and Utilization Project (HCUP). Agency for Healthcare Research and Quality. Updated March 2017. www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed January 18, 2018. 18 Compton WM, Jones CM, Baldwin GT. Relationship between nonmedical prescription-opioid use and heroin use. The New England Journal of Medicine. 2016;374:154-63. 19 Goodman RA, Posner SF, Huang ES, Parekh AK, Koh HK. Defining and measuring chronic conditions: imperatives for research, policy, program and practice. Preventing Chronic Disease. 2013;10:120239. 20 Steiner CA, Friedman B. Hospital utilization, costs, and mortality for adults with multiple chronic conditions, Nationwide Inpatient Sample, 2009. Preventing Chronic Disease. 2013;10:120292. 21 Agency for Healthcare Research and Quality. HCUP Cost-to-Charge Ratio (CCR) Files. Healthcare Cost and Utilization Project (HCUP). 2001-2015. Agency for Healthcare Research and Quality. Updated December 2017. www.hcup-us.ahrq.gov/db/state/costtocharge.jsp. Accessed January 18, 2018. 22 U.S. Bureau of Economic Analysis. GDP & Personal Income Tables, Table 1.1.4. Price Indexes for Gross Domestic Product. www.bea.gov/iTable/iTable.cfm?reqid=19&step=2#reqid=19&step=3&isuri=1&1910=x&0=-99&1921=survey&1903=4&1904=2000&1905=2016&1906=a&1911=0. Accessed March 26, 2018. 23 U.S. Bureau of Labor, Bureau of Labor Statistics, Table 24. Historical Consumer Price Index for All Urban Consumers (CPI-U): U. S. City Average, All Items. www.bls.gov/cpi/tables/supplemental-files/historical-cpi-u-201803.pdf. Accessed April 17, 2018. 24 Claritas. Claritas Demographic Profile by ZIP Code. www.claritas360.claritas.com/mybestsegments/. |
| Internet Citation: Statistical Brief #244. Healthcare Cost and Utilization Project (HCUP). September 2018. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb244-Opioid-Inpatient-Stays-ED-Visits-Older-Adults.jsp?utm_source=ahrq&utm_medium=en1&utm_term=&utm_content=1&utm_campaign=ahrq_en1_29_2019. |
| Are you having problems viewing or printing pages on this website? |
| If you have comments, suggestions, and/or questions, please contact hcup@ahrq.gov. |
| Privacy Notice, Viewers & Players |
| Last modified 9/12/18 |