STATISTICAL BRIEF #243 |
September 2018
Kathryn R. Fingar, Ph.D., M.P.H., Megan M, Hambrick, M.S.W., Kevin C. Heslin, Ph.D., and Jennifer E. Moore, Ph.D., R.N. Introduction Severe maternal morbidity is defined as including unexpected outcomes of labor and delivery that result in significant short- or long-term consequences to a woman's health.1 Often called near-misses, deliveries involving severe maternal morbidity generally include life-threatening conditions, such as acute myocardial infarction, pulmonary embolism, or sepsis.2 It has been found that rates of severe maternal morbidity are steadily increasing in the United States.3 Furthermore, severe maternal morbidity disproportionately affects minority and low-income pregnant women, especially non-Hispanic Black women and those with Medicaid coverage.4,5 Recent studies have found that rising rates of severe maternal morbidity may be attributed to changes in the overall health of women, leading to increased complications including maternal mortality.6,7,8 Among pregnancy-related deaths in the United States between 2011 and 2013, 15.1 percent were caused by cardiovascular disease, 14.5 percent by noncardiovascular diseases, 12.7 percent by infection and sepsis, and 11.4 percent by hemorrhage.9 Disparities in mortality by race/ethnicity also are highest among non-Hispanic Black women at 43.5 deaths per 100,000 live births, compared with 12.7 among White women.10 This Healthcare Cost and Utilization Project (HCUP) Statistical Brief presents trends and disparities in delivery hospitalizations involving severe maternal morbidity from 2006 through the third quarter of 2015. The fourth quarter of 2015 is excluded because of the transition of the International Classification of Diseases coding system from the 9th to the 10th revision.11 This Statistical Brief defines severe maternal morbidity using a standardized measure containing 21 indicators that was developed by the Centers for Disease Control and Prevention.12 These 21 indicators of severe maternal morbidity include conditions (e.g., renal failure, sepsis), as well as procedures performed during the hospital stay (e.g., blood transfusion, hysterectomy), that may or may not have resulted in in-hospital death. First, trends in severe maternal morbidity overall and for each indicator of severe maternal morbidity are presented. Some conditions may be more likely to result in procedural intervention. Thus, the prevalence of the most common procedures indicating severe maternal morbidity—blood transfusion and hysterectomy—are examined among deliveries with a condition defined as a severe maternal morbidity. Second, patient and hospital characteristics are compared across deliveries with and without severe maternal morbidity in 2015. Finally, disparities in rates of severe maternal morbidity and in-hospital mortality are examined over time by race/ethnicity. All differences between estimates noted in the text are 10 percent or greater. Findings Trends in and types of severe maternal morbidity, 2006-2015 Figure 1 displays the rate of deliveries involving severe maternal morbidity per 10,000 delivery hospitalizations from 2006 through 2015. Because blood transfusion represents the most common indicator of severe morbidity,13 trends are presented for blood transfusions (with or without other indicators of severe maternal morbidity) and for other indicators of severe maternal morbidity (with or without blood transfusion). If a delivery involved blood transfusion and 1 of the other 20 indicators of severe maternal morbidity, the delivery was counted in both categories. |
|
|
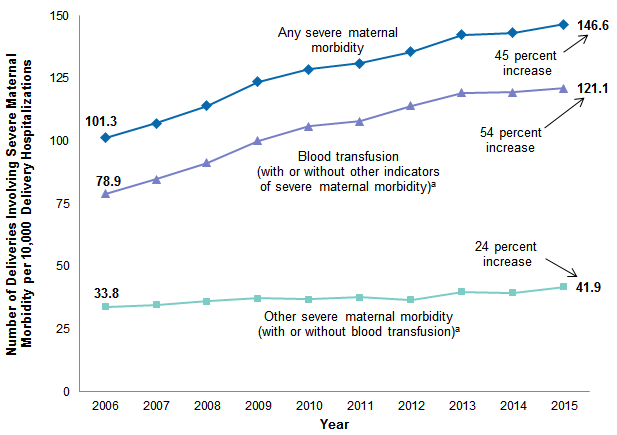
Figure 1. Trends in delivery hospitalizations involving severe maternal morbidity, 2006-2015
a If a delivery involved blood transfusion and 1 of the other 20 types of severe maternal morbidity, the delivery was counted in both categories. Line graph that shows the number of deliveries involving severe maternal morbidity per 10,000 delivery hospitalizations from 2006 through 2015. Any severe maternal morbidity: increased steadily from 101.3 in 2006 to 146.6 in 2015, for a 146.6% increase. Blood transfusion (with or without other indicators of several material morbidity): increased steadily from 78.9 in 2006 to 121.1 in 2015, for a 54% increase. Other severe maternal morbidity (with or without blood transfusion): increased steadily from 33.8 in 2006 to 41.9 in 2015, for a 24% increase. |
|
| Table 1. Trends in delivery hospitalizations involving severe maternal morbidity, overall and for each indicator of severe maternal morbidity, 2006 and 2015 | |||||
| Indicators of severe maternal morbidity | Deliveries involving any severe maternal morbidity, % | Rate per 10,000 deliveries | Cumulative percentage change in rate | ||
|---|---|---|---|---|---|
| 2006 | 2015 | 2006 | 2015 | ||
| Any severe maternal morbidity, considering and not considering blood transfusions | |||||
| Any severe maternal morbidity | 100.0 | 100.0 | 101.3 | 146.6 | 45 |
| Blood transfusion (with or without other indicators of severe maternal morbidity)a | 77.9 | 82.6 | 78.9 | 121.1 | 54 |
| Other indicators of severe maternal morbidity (with or without blood transfusion)a | 33.4 | 28.6 | 33.8 | 41.9 | 24 |
| Other indicators of severe maternal morbidity | |||||
| Acute renal failure | 2.7 | 4.4 | 2.8 | 6.5 | 134 |
| Shock | 1.8 | 2.9 | 1.9 | 4.3 | 133 |
| Ventilation | 0.6 | 0.8 | 0.6 | 1.2 | 105 |
| Sepsis | 2.5 | 3.6 | 2.6 | 5.2 | 104 |
| Aneurysm | 0.1 | 0.1 | 0.1 | 0.1 | 99 |
| Adult respiratory distress syndrome | 4.1 | 4.0 | 4.2 | 5.9 | 42 |
| Disseminated intravascular coagulation | 7.8 | 7.5 | 7.9 | 11.0 | 39 |
| Hysterectomy | 8.2 | 7.5 | 8.3 | 11.0 | 32 |
| Cardiac arrest/ventricular fibrillation | 0.6 | 0.5 | 0.6 | 0.7 | 26 |
| Temporary tracheostomy | 0.1 | 0.1 | 0.1 | 0.1 | 14 |
| Conversion of cardiac rhythm | 0.7 | 0.5 | 0.7 | 0.7 | 13 |
| Amniotic fluid embolism | 0.3 | 0.2 | 0.3 | 0.3 | 11 |
| Sickle cell disease with crisis | 0.9 | 0.6 | 1.0 | 0.9 | 0 |
| Pulmonary edema/acute heart failure | 4.3 | 2.2 | 4.3 | 3.2 | -25 |
| Air and thrombotic embolism | 1.3 | 0.7 | 1.3 | 1.0 | -26 |
| Eclampsia | 4.3 | 2.1 | 4.3 | 3.1 | -28 |
| Puerperal cerebrovascular disorders | 1.5 | 0.7 | 1.5 | 1.0 | -32 |
| Acute myocardial infarction | 0.2 | 0.1 | 0.2 | 0.1 | -36 |
| Severe anesthesia complications | 1.0 | 0.3 | 1.0 | 0.5 | -51 |
| Heart failure/arrest during surgery | 0.9 | 0.3 | 0.9 | 0.4 | -53 |
| Notes: There were 44,000 deliveries with any severe maternal morbidity in 2006 and 43,800 deliveries with any severe maternal morbidity in the first 3 quarters of 2015 (rounded to the nearest hundred). Percentage change was calculated from unrounded rates; thus, the rounded rates may appear the same in 2006 and 2015 but still represent a cumulative change from 2006 through 2015 based on the unrounded rates. If a delivery involved multiple indicators of severe maternal morbidity, it was counted in each category. a If a delivery involved blood transfusion and 1 of the other 20 indicators of severe maternal morbidity, the delivery was counted in both categories. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), State Inpatient Databases (SID), 2006 and 2015 quarters 1-3, weighted to provide national estimates using the same methodology as the Nationwide Inpatient Sample (NIS), 2011 and prior years | |||||
|
|
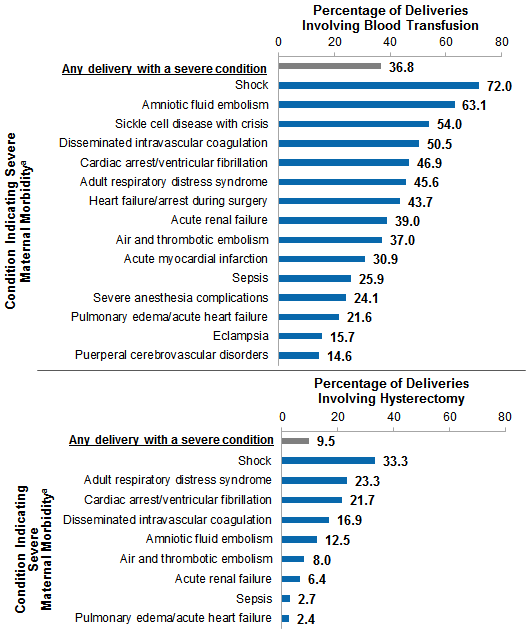
Figure 2. Percentage of deliveries involving blood transfusion or hysterectomy among deliveries with a condition indicating severe maternal morbidity, 2015
a Conditions are not shown if there were fewer than 11 deliveries with the condition that involved blood transfusion or hysterectomy in 2015; however; these conditions are included in the category of Any delivery with a severe condition. Bar chart that shows the percentage of deliveries involving blood transfusion or hysterectomy for conditions indicating severe maternal morbidity by condition in 2015. Deliveries involving blood transfusion: any delivery with a severe condition, 36.8; shock, 72.0; amniotic fluid embolism, 63.1; sickle cell disease with crisis, 54.0; disseminated intravascular coagulation, 50.5; cardiac arrest/ventricular fibrillation, 46.9; adult respiratory distress syndrome, 45.6; heart failure/arrest during surgery, 43.7; acute renal failure, 39.0; air and thrombotic embolism, 37.0; acute myocardial infarction, 30.9; sepsis, 25.9; severe anesthesia complications, 24.1; pulmonary edema/acute heart failure, 21.6; eclampsia, 15.7; puerperal cerebrovascular disorders, 14.6. Deliveries involving hysterectomy: any delivery with a severe condition, 9.5; shock, 33.3; adult respiratory distress syndrome, 23.3; cardiac arrest/ventricular fibrillation, 21.7; disseminated intravascular coagulation, 16.9; amniotic fluid embolism, 12.5; air and thrombotic embolism, 8.0; acute renal failure, 6.4; sepsis, 2.7; pulmonary edema/acute heart failure, 2.4. |
Table 2 presents characteristics of deliveries with and without a severe maternal morbidity during the first 3 quarters of 2015. The rate of severe maternal morbidity per 10,000 total delivery hospitalizations also is presented. Hereinafter, this Statistical Brief presents data on any severe maternal morbidity, involving any of the 21 indicators discussed above. |
| Table 2. Characteristics of deliveries with and without any severe maternal morbidity, 2015 | |||
| Characteristic | Deliveries with any severe maternal morbidity, % | Deliveries with no severe maternal morbidity, % | Rate of any severe maternal morbidity per 10,000 total delivery hospitalizations |
|---|---|---|---|
| Patient characteristic | |||
| Age group, years | |||
| <20 | 8.5 | 6.0 | 206.3 |
| 20-29 | 46.6 | 50.2 | 136.3 |
| 30-39 | 39.7 | 40.8 | 143.0 |
| 40+ | 5.1 | 3.0 | 248.0 |
| Primary expected payer | |||
| Medicaid | 51.4 | 42.9 | 175.0 |
| Private insurance | 42.1 | 51.3 | 120.8 |
| Uninsured | 3.1 | 2.6 | 176.5 |
| Other (including Medicare) | 3.4 | 3.2 | 153.9 |
| Community income | |||
| Quartile 1 (poorest) | 36.4 | 29.9 | 177.7 |
| Quartile 2 | 22.8 | 23.0 | 145.6 |
| Quartile 3 | 22.1 | 24.6 | 131.9 |
| Quartile 4 (wealthiest) | 18.7 | 22.5 | 122.2 |
| Location of residence | |||
| Large metropolitan | 63.4 | 60.3 | 154.0 |
| Small metropolitan | 24.0 | 26.4 | 133.5 |
| Micropolitan | 7.6 | 8.0 | 140.0 |
| Rural (noncore) | 4.9 | 5.2 | 138.1 |
| Hospital characteristic | |||
| Safety-net hospital | |||
| Yes | 43.6 | 35.1 | 181.8 |
| No | 56.4 | 64.9 | 127.5 |
| Minority-serving hospital | |||
| Yes | 53.4 | 44.3 | 176.3 |
| No | 46.6 | 55.7 | 123.0 |
| Teaching status | |||
| Teaching hospital | 70.6 | 66.7 | 155.1 |
| Nonteaching hospital | 29.4 | 33.3 | 129.7 |
| Ownership | |||
| Private for-profit | 14.6 | 14.5 | 147.8 |
| Private nonprofit | 69.7 | 73.2 | 139.6 |
| Public | 15.7 | 12.3 | 187.1 |
| Region | |||
| Northeast | 17.9 | 15.8 | 165.4 |
| Midwest | 16.7 | 21.1 | 116.3 |
| South | 44.4 | 39.7 | 163.6 |
| West | 21.1 | 23.4 | 132.4 |
| Notes: In the first 3 quarters of 2015, there were 2.9 million deliveries without severe maternal morbidity and 43,800 deliveries with any severe maternal morbidity (rounded to the nearest hundred). Percentages add to 100 percent within the column and were calculated from unrounded counts of observations with nonmissing values. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), State Inpatient Databases (SID), 2015 quarters 1-3, weighted to provide national estimates using the same methodology as the Nationwide Inpatient Sample (NIS), 2011 and prior years | |||
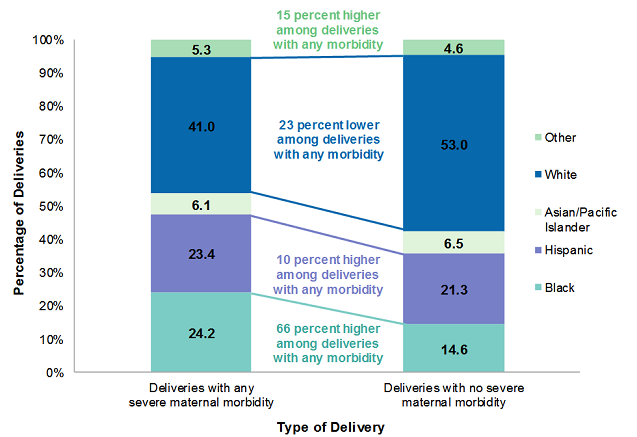
Figure 3 displays the distribution of race/ethnicity among deliveries with any severe maternal morbidity compared with all other deliveries, in the first 3 quarters of 2015. |
|
Figure 3. The distribution of race/ethnicity among delivery hospitalizations, according to whether the delivery involved any severe maternal morbidity, 2015
Notes: In the first 3 quarters of 2015, there were 2.9 million deliveries without severe maternal morbidity and 43,800 deliveries with any severe maternal morbidity (rounded to the nearest hundred). Percentages in the figure are based on unrounded counts. Bar chart that shows the percentage of deliveries with and without severe maternal morbidity by race/ethnicity in 2015. Other: deliveries with any severe maternal morbidity, 5.3; deliveries with no severe maternal morbidity, 4.6—15% higher among deliveries with any morbidity. White: deliveries with any severe maternal morbidity, 41.0; deliveries with no severe maternal morbidity, 53.0—23% lower among deliveries with any morbidity. Asian/Pacific Islander: deliveries with any severe maternal morbidity, 6.1; deliveries with no severe maternal morbidity, 6.5. Hispanic: deliveries with any severe maternal morbidity, 23.4; deliveries with no severe maternal morbidity, 21.3—10 percent higher among deliveries with any morbidity. Black: deliveries with any severe maternal morbidity, 24.2; deliveries with no severe maternal morbidity, 14.6—66 percent higher among deliveries with any morbidity. |
|
|
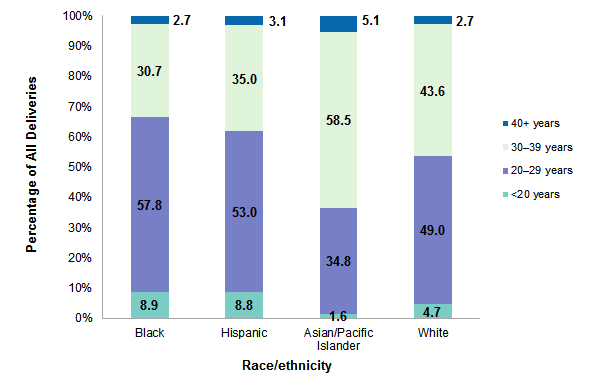
Figure 4. The distribution of age of all delivery hospitalizations, by patient race/ethnicity, 2015
Notes: In the first 3 quarters of 2015, there were 440,900 deliveries among Blacks, 636,400 deliveries among Hispanics, 192,800 deliveries among Asian/Pacific/Islanders, and 1.6 million deliveries among Whites (rounded to the nearest hundred). Percentages in the figure are based on unrounded counts. Other races/ethnicities are not shown. Bar chart that shows the percentage of all delivery hospitalizations for each age group by race/ethnicity in 2015. Black: 40+ years, 2.7; 30-39 years, 30.7; 20-29 years, 57.8; <20 years, 8.9. Hispanic: 40+ years, 3.1; 30-39 years, 35.0; 20-29 years, 53.0; <20 years, 8.8. Asian/Pacific Islander: 40+ years, 5.1; 30-39 years, 58.5; 20-29 years, 34.8; <20 years, 1.6. White: 40+ years, 2.7; 30-39 years, 43.6; 20-29 years, 49.0; <20 years, 4.7.
|
|
|
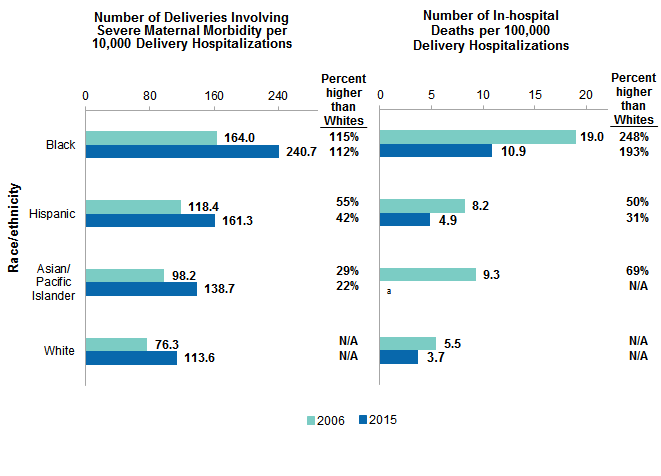
Figure 5. Rates of severe maternal morbidity and in-hospital deaths among delivery hospitalizations, by patient race/ethnicity, 2006 and 2015
Abbreviation: N/A, not applicable Bar chart that shows the number of deliveries involving severe maternal morbidity and the number of in-hospital deaths per 10,000 delivery hospitalizations by patient race/ethnicity in 2006 and 2015. Number of deliveries involving severe maternal morbidity per 10,000 delivery hospitalizations: Black: 2006, 164.0 (115% higher than Whites); 2015, 240.7 (112% higher than Whites). Hispanic: 2006, 118.4 (55% higher than Whites); 2015, 161.3 (42% higher than Whites). Asian/Pacific Islander: 2006, 98.2 (29% higher than Whites); 2015, 138.7 (22% higher than Whites). White: 2006, 76.3; 2015, 113.6. Number of in-hospital deaths per 10,000 delivery hospitalizations: Black: 2006, 19.0 (248% higher than Whites); 2015, 10.9 (193% higher than Whites). Hispanic: 2006, 8.2 (50% higher than Whites); 2015, 4.9 (31% higher than Whites). Asian/Pacific Islander: 2006, 9.3 (69% higher than Whites); 2015, suppressed because of cell size <11. White: 2006, 5.5; 2015, 3.7.
|
About Statistical Briefs Healthcare Cost and Utilization Project (HCUP) Statistical Briefs provide basic descriptive statistics on a variety of topics using HCUP administrative health care data. Topics include hospital inpatient, ambulatory surgery, and emergency department use and costs, quality of care, access to care, medical conditions, procedures, and patient populations, among other topics. The reports are intended to generate hypotheses that can be further explored in other research; the reports are not designed to answer in-depth research questions using multivariate methods. Data Source The estimates in this Statistical Brief are based upon data from HCUP. An analysis file was used that was derived from the HCUP State Inpatient Databases (SID) from 2006 through the third quarter of 2015. This file was weighted to provide national estimates calculated with the same methodology as the Nationwide Inpatient Sample (NIS) in 2011 and prior years. This is the same file used for the Agency for Research and Quality (AHRQ) National Healthcare Quality and Disparities Report (QDR). The fourth quarter of 2015 is excluded because of the transition of the International Classification of Diseases coding system from the 9th to the 10th revision.15 Definitions Diagnoses, procedures, ICD-9-CM, and diagnosis-related groups (DRGs) The principal diagnosis is that condition established after study to be chiefly responsible for the patient's admission to the hospital. Secondary diagnoses are concomitant conditions that coexist at the time of admission or develop during the stay. All-listed diagnoses include the principal diagnosis plus these additional secondary conditions. All-listed procedures include all procedures performed during the hospital stay, whether for definitive treatment or for diagnostic or exploratory purposes. The first-listed procedure is the procedure that is listed first on the discharge record. Inpatient data define this as the principal procedure—the procedure that is performed for definitive treatment rather than for diagnostic or exploratory purposes (i.e., the procedure that was necessary to take care of a complication). ICD-9-CM is the International Classification of Diseases, Ninth Revision, Clinical Modification, which assigns numeric codes to diagnoses and procedures. There are approximately 14,000 ICD-9-CM diagnosis codes. There are approximately 4,000 ICD-9-CM procedure codes. DRGs comprise a patient classification system that categorizes patients into groups that are clinically coherent and homogeneous with respect to resource use. DRGs group patients according to diagnosis, type of treatment (procedure), age, and other relevant criteria. Each hospital stay has one assigned DRG. Case definition The ICD-9-CM codes defining severe maternal morbidity (with or without in-hospital death) include the diagnosis and procedure codes listed in Table 3. The definition was based on all-listed codes on the delivery hospitalization record, using methods developed by the Centers for Disease Control and Prevention.16 |
| Table 3. Diagnosis and procedure codes used to define 21 indicators of maternal morbidity as specified by the Centers for Disease Control and Prevention | ||
| Severe maternal morbidity indicator | Diagnosis or procedure | ICD-9-CM code |
|---|---|---|
| Acute myocardial infarction | Diagnosis | 410.xx |
| Aneurysm | Diagnosis | 441.xx |
| Acute renal failure | Diagnosis | 584.5, 584.6, 584.7, 584.8, 584.9, 669.3x |
| Adult respiratory distress syndrome | Diagnosis | 518.5x, 518.81 518.82 518.84, 799.1 |
| Amniotic fluid embolism | Diagnosis | 673.1x |
| Cardiac arrest/ventricular fibrillation | Diagnosis | 427.41, 427.42, 427.5 |
| Disseminated intravascular coagulation | Diagnosis | 286.6, 286.9, 666.3x |
| Eclampsia | Diagnosis | 642.6x |
| Heart failure/arrest during surgery or procedure | Diagnosis | 997.1 |
| Puerperal cerebrovascular disorders | Diagnosis | 430.xx, 431.xx, 432.xx, 433.xx, 434.xx, 436.xx, 437.xx, 671.5x, 674.0x, 997.02 |
| Puerperal cerebrovascular disorders | Diagnosis | 430.xx, 431.xx, 432.xx, 433.xx, 434.xx, 436.xx, 437.xx, 671.5x, 674.0x, 997.02 |
| Severe anesthesia complications | Diagnosis | 668.0x, 668.1x, 668.2x |
| Sepsis | Diagnosis | 038.xx, 995.91, 995.92, 670.2x |
| Shock | Diagnosis | 669.1x, 785.5x, 995.0, 995.4, 998.0x |
| Sickle cell disease with crisis | Diagnosis | 282.42, 282.62, 282.64, 282.69 |
| Air and thrombotic embolism | Diagnosis | 415.1x, 673.0x, 673.2x, 673.3x, 673.8x |
| Blood transfusion | Procedure | 99.0x |
| Conversion of cardiac rhythm | Procedure | 99.6x |
| Hysterectomy | Procedure | 68.3x-68.9x |
| Temporary tracheostomy | Procedure | 31.1 |
| Ventilation | Procedure | 93.90, 96.01, 96.02, 96.03, 96.05 |
| Abbreviation: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification | ||
If the delivery involving severe maternal morbidity did not involve a procedure listed in Table 3 or did not result in death during the delivery hospitalization, it was counted as involving severe maternal morbidity only if the length of stay was—
In-hospital deaths (with or without severe maternal morbidity) were defined as delivery records with a disposition indicating that the woman died. Delivery hospitalizations were defined using an expanded definition developed by Kuklina et al. (2008), as shown in Table 4.17 |
| Table 4. Enhanced delivery hospitalization identification method | |
| Description | Codes |
|---|---|
| Outcome of delivery diagnosis | ICD-9-CM = V27.x |
| Normal delivery diagnosis | ICD-9-CM = 650 |
| DRG delivery codes | Before October 1, 2007: DRG = 370 (complicated cesarean section) DRG = 371 (uncomplicated cesarean section) DRG = 372 (complicated vaginal delivery) DRG = 373 (uncomplicated vaginal delivery) DRG = 374 (uncomplicated vaginal delivery with sterilization and/or dilation and curettage) DRG = 375 (vaginal delivery with operation room procedure except sterilization and/or dilation and curettage) On or after October 1, 2007: MS-DRG = 765 (complicated cesarean section) MS-DRG = 766 (uncomplicated cesarean section) MS-DRG = 767 (uncomplicated vaginal delivery with sterilization and/or dilation and curettage) MS-DRG = 768 (vaginal delivery with operation room procedure except sterilization and/or dilation and curettage) MS-DRG = 774 (complicated vaginal delivery) MS-DRG = 775 (uncomplicated vaginal delivery) |
| Selected delivery related procedures | ICD-9-CM = 72.0, 72.1, 72.21, 72.29, 72.31, 72.39, 72.4, 72.6 (forceps) ICD-9-CM = 72.51, 72.52, 72.53, 72.54 (breech extraction) ICD-9-CM = 72.71, 72.79 (vacuum extraction) ICD-9-CM = 72.8, 72.9 (other specified and unspecified delivery) ICD-9-CM = 73.22 (internal and combined version and extraction) ICD-9-CM = 73.59 (other manually assisted deliveries) ICD-9-CM = 73.6 (episiotomy) ICD-9-CM = 74.0, 74.1, 74.2, 74.4, 74.99 (cesarean section) |
| Exclusions | ICD-9-CM = 630 (hydatidiform mole diagnosis) ICD-9-CM = 631 (other abnormal product of conception diagnosis) ICD-9-CM = 633.x (ectopic pregnancy diagnosis) ICD-9-CM = 632, 634.xx, 635.xx, 636.xx, 637.xx, 638.x, 639.x (abortion diagnosis) ICD-9-CM = 69.01, 69.51, 74.91, 75.0 (abortion procedure) |
| Abbreviations: DRG, diagnosis-related group; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; MS-DRG, Medicare severity diagnosis-related group | |
Additionally, both the denominator and numerator were limited to deliveries at community, nonrehabiliation hospitals, to women aged 12-55 years, and to records with sex equal to female.
Types of hospitals included in the HCUP National (Nationwide) Inpatient Sample The National (Nationwide) Inpatient Sample (NIS) is based on data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). The NIS includes obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Beginning in 2012, long-term acute care hospitals are also excluded. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay will be included in the NIS. Types of hospitals included in HCUP State Inpatient Databases This analysis used State Inpatient Databases (SID) limited to data from community hospitals, which are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). Community hospitals include obstetrics and gynecology, otolaryngology, orthopedic, cancer, pediatric, public, and academic medical hospitals. Excluded for this analysis are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. However, if a patient received long-term care, rehabilitation, or treatment for a psychiatric or chemical dependency condition in a community hospital, the discharge record for that stay was included in the analysis. Unit of analysis The unit of analysis is the hospital discharge (i.e., the hospital stay), not a person or patient. This means that a woman who delivers multiple times in 1 year will be counted each time as a separate discharge from the hospital. Location of patients' residence Place of residence is based on a simplified adaptation of the Urban Influence Codes (UIC) developed by the United States Department of Agriculture (USDA) Economic Research Service (ERS). Starting with 2014 data, the county-level designation is based on the 2013 version of the UIC. Prior to 2014, the categorization was based on the 2003 version of the UIC. The 12 categories of the UIC are combined into 4 broader categories that differentiate between large metropolitan counties (include one or more urbanized areas with at least 1 million residents), small metropolitan counties (include one or more urbanized areas with 50,000-999,999 residents), micropolitan counties (include at least one urbanized area with 10,000-49,999 residents), and nonurban residual counties (rural). Community-level income Community-level income is based on the median household income of the patient's ZIP Code of residence. Quartiles are defined so that the total U.S. population is evenly distributed. Cut-offs for the quartiles are determined annually using ZIP Code demographic data obtained from Claritas, a vendor that adds value to data from the U.S. Census Bureau.18 The income quartile is missing for patients who are homeless or foreign. Payer Payer is the expected payer for the hospital stay. To make coding uniform across all HCUP data sources, payer combines detailed categories into general groups:
For this Statistical Brief, when more than one payer is listed for a hospital discharge, the first-listed payer is used. Region Region is one of the four regions defined by the U.S. Census Bureau:
Data on Hispanic ethnicity are collected differently among the States and also can differ from the census methodology of collecting information on race (White, Black, Asian/Pacific Islander, American Indian/Alaska Native, Other [including mixed race]) separately from ethnicity (Hispanic, non-Hispanic). State data organizations often collect Hispanic ethnicity as one of several categories that include race. Therefore, for multistate analyses, HCUP creates the combined categorization of race and ethnicity for data from States that report ethnicity separately. When a State data organization collects Hispanic ethnicity separately from race, HCUP uses Hispanic ethnicity to override any other race category to create a Hispanic category for the uniformly coded race/ethnicity data element, while also retaining the original race and ethnicity data. This Statistical Brief reports race/ethnicity for the following categories: Hispanic, non-Hispanic White, non-Hispanic Black, non-Hispanic Asian/Pacific Islander, and non-Hispanic Other. Safety-net hospital Using data from all community, nonrehabilitation hospitals in the State Inpatient Databases (SID), the number of discharges paid by Medicaid or that were uninsured was divided by the total number of discharges at each hospital. Hospitals were ranked by this percentage, and those hospitals falling in the top 25 percent were defined as safety-net hospitals. Remaining hospitals were defined as nonsafety-net hospitals. Minority-serving hospital Using data from all community, nonrehabilitation hospitals in the State Inpatient Databases (SID) with reliable reporting of race/ethnicity, the number of discharges among patients that were not White was divided by the total number of discharges at each hospital. Hospitals were ranked by this percentage, and those hospitals falling in the top 25 percent were defined as minority-serving hospitals. Remaining hospitals were defined as nonminority-serving hospitals. Teaching hospital Teaching hospitals are hospitals that are members of the University HealthSystem Consortium or the Council of Teaching Hospitals. About HCUP The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of health care databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level health care data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to health care programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska Department of Health and Social Services Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association Delaware Division of Public Health District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi State Department of Health Missouri Hospital Industry Data Institute Montana Hospital Association Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Department of Health and Human Resources, West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About the NIS The HCUP National (Nationwide) Inpatient Sample (NIS) is a nationwide database of hospital inpatient stays. The NIS is nationally representative of all community hospitals (i.e., short-term, non-Federal, nonrehabilitation hospitals). The NIS includes all payers. It is drawn from a sampling frame that contains hospitals comprising more than 95 percent of all discharges in the United States. The vast size of the NIS allows the study of topics at the national and regional levels for specific subgroups of patients. In addition, NIS data are standardized across years to facilitate ease of use. Over time, the sampling frame for the NIS has changed; thus, the number of States contributing to the NIS varies from year to year. The NIS is intended for national estimates only; no State-level estimates can be produced. The 2012 NIS was redesigned to optimize national estimates. The redesign incorporates two critical changes:
About the SID The HCUP State Inpatient Databases (SID) are hospital inpatient databases from data organizations participating in HCUP. The SID contain the universe of the inpatient discharge abstracts in the participating HCUP States, translated into a uniform format to facilitate multistate comparisons and analyses. Together, the SID encompass more than 95 percent of all U.S. community hospital discharges. The SID can be used to investigate questions unique to one State, to compare data from two or more States, to conduct market-area variation analyses, and to identify State-specific trends in inpatient care utilization, access, charges, and outcomes. About the QDR The National Healthcare Quality and Disparities Report (QDR) measures and tracks trends in quality and disparities in seven key areas of health care: patient safety, person-centered care, care coordination, effective treatment, healthy living, care affordability, and access to health care. The QDR is an annual report that was commissioned by Congress in 1999 and first published in 2003. Beginning with the 2014 report, findings that previously appeared in two separate reports (the National Healthcare Quality Report and the National Healthcare Disparities Report) have been integrated into a single document that provides a comprehensive overview of the quality of health care received by the general population and disparities in care experienced by different racial, ethnic, and socioeconomic groups. Information on individual measures are available through chartbooks, which are posted periodically. The QDR is designed and produced by AHRQ, with support from the Department of Health and Human Services (HHS) and private sector partners. For More Information For other information on pregnancy and childbirth, refer to the HCUP Statistical Briefs located at www.hcup-us.ahrq.gov/reports/statbriefs/sb_pregnancy.jsp. For additional HCUP statistics, visit:
For a detailed description of HCUP and more information on the design of the National (Nationwide) Inpatient Sample (NIS) and State Inpatient Databases (SID), please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the National (Nationwide) Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated February 2018. www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed February 12, 2018. Agency for Healthcare Research and Quality. Overview of the State Inpatient Databases (SID). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated April 2017. www.hcup-us.ahrq.gov/sidoverview.jsp. Accessed January 18, 2018. Suggested Citation Fingar KF (IBM Watson Health), Hambrick MM (AHRQ), Heslin KC (AHRQ), Moore JE (Institute for Medicaid Innovation). Trends and Disparities in Delivery Hospitalizations Involving Severe Maternal Morbidity, 2006-2015. HCUP Statistical Brief #243. September 2018. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb243-Severe-Maternal-Morbidity-Delivery-Trends-Disparities.pdf. Acknowledgments The authors would like to acknowledge the contributions of Minya Sheng of IBM Watson Health, Marguerite Barrett of M.L. Barrett, Inc., Andrea A. Creanga of Johns Hopkins University, and Brian T. Bateman of Harvard University. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of health care in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:Virginia Mackay-Smith, Acting Director Center for Delivery, Organization, and Markets Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 This Statistical Brief was posted online on September 4. 2018. 1 American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine, Kilpatrick SK, Ecker JL. Severe maternal morbidity: screening and review. American Journal of Obstetrics & Gynecology. 2016;215(3):B17-22. 2 Geller SE, Rosenberg D, Cox SM, Kilpatrick S. Defining a conceptual framework for near-miss maternal morbidity. Journal of the American Medical Women's Association. 2002;57(3):135-9. 3 Centers for Disease Control and Prevention. Severe Maternal Morbidity in the United States. November 2017. www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html. Accessed April 24, 2018. 4 Admon LK, Windelman TNA, Moniz MH, Davis MM, Heisler M, Dalton VK. Disparities in chronic conditions among women hospitalized for delivery in the United States, 2005-2014. Obstetrics & Gynecology. 2017;130(6):1319-26. 5 Creanga AA, Bateman BT, Kuklina EV, Callaghan WM. Racial and ethnic disparities in severe maternal morbidity: a multistate analysis, 2008-2010. American Journal of Obstetrics & Gynecology. 2014;210(5):435.e1-8. 6 Campbell KH, Savitz D, Werner EF, Pettker CM, Goffman D, Chazotte C, et al. Maternal morbidity and risk of death at delivery hospitalization. Obstetrics & Gynecology. 2013;122(3):627-33. 7 Martin JA, Hamilton BE, Osterman MJK, Driscoll AK, Matthews TJ. Births: final data for 2015. Centers for Disease Control and Prevention. National Vital Statistics Reports. 2017;66(1):1-70. 8 Small MJ, James AH, Kershaw T, Thames B, Gunatilake R, Brown H. Near-miss maternal mortality: cardiac dysfunction as the principal cause of obstetric intensive care unit admissions. Obstetrics & Gynecology. 2012;119(2):250-5. 9 Centers for Disease Control and Prevention. Pregnancy Mortality Surveillance System. November 2017. www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html. Accessed April 24, 2018. 10 Ibid. 11 Barrett ML, Heslin KC, Yoon F, Moore BJ. Case Study: National Healthcare Quality and Disparities Report (QDR) Sensitivity Analysis on Developing AHRQ Quality Indicator Estimates for 2015 Using Only ICD-9-CM Data. April 7, 2017. Agency for Healthcare Research and Quality. www.hcup-us.ahrq.gov/datainnovations/CaseStudy_QDRanalysis04072017.pdf. Accessed April 24, 2018. 12 Centers for Disease Control and Prevention. Severe Maternal Morbidity in the United States. November 2017. www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html. Accessed April 24, 2018. 13 Centers for Disease Control and Prevention. Severe Maternal Morbidity in the United States. November 2017. www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html. Accessed April 24, 2018. 14 Creanga AA, Bateman BT, Kuklina EV, Callaghan WM. Racial and ethnic disparities in severe maternal morbidity: a multistate analysis, 2008-2010. American Journal of Obstetrics & Gynecology. 2014;210(5):435.e1-8. 15 Barrett ML, Heslin KC, Yoon F, Moore BJ. Case Study: National Healthcare Quality and Disparities Report (QDR) Sensitivity Analysis on Developing AHRQ Quality Indicator Estimates for 2015 Using Only ICD-9-CM Data. April 7, 2017. Agency for Healthcare Research and Quality. www.hcup-us.ahrq.gov/datainnovations/CaseStudy_QDRanalysis04072017.pdf. Accessed April 24, 2018. 16 Centers for Disease Control and Prevention. Severe Maternal Morbidity in the United States. November 2017. www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html. Accessed April 24, 2018. 17 Kuklina EV, Whiteman MK, Hillis SD, Jamieson DJ, Meikle SF, Posner SF, et al. An enhanced method for identifying obstetric deliveries: implications for estimating maternal morbidity. Maternal Child Health Journal. 2008;12(4):469-77 18 Claritas. Claritas Demographic Profile by ZIP Code. https://claritas360.claritas.com/mybestsegments/. |