STATISTICAL BRIEF #221 |
February 2017
H. Joanna Jiang, Ph.D., Audrey J. Weiss, Ph.D., and Marguerite L. Barrett, M.S. Introduction Over the last several years, healthcare stakeholders have paid increasing attention to issues specific to high-need, high-cost patients who constitute a very small percentage of the population but account for a disproportionally high amount of healthcare utilization. These patients, dubbed super-utilizers, represent a broad spectrum of demographic and clinical characteristics and socioeconomic conditions. Programs designed to improve care for super-utilizers need to be tailored to the specific needs of the different subgroups of these patients. As part of this effort, it is important to examine differences in utilization patterns among different types of super-utilizers, in comparison to national benchmarks. In a series of Statistical Briefs, the Agency for Health Care Research and Quality (AHRQ) is providing descriptive information on demographic and clinical characteristics of super-utilizers of hospital services, using nationwide data from the Healthcare Cost and Utilization Project (HCUP).1,2 For example, AHRQ reported that, in 2012, congestive heart failure and septicemia were among the 10 most common reasons for hospitalization among super-utilizers across all payers.3 Mental health disorders and diabetes with complications also were common reasons for hospitalization among super-utilizers aged 1-64 years.4 This HCUP Statistical Brief extends AHRQ's earlier work on super-utilizers by shifting focus from hospital inpatient stays to emergency department (ED) visits. In this Statistical Brief, we limited our analysis to ED visits among patients who were treated in the ED and then released from the ED, transferred to another type of nonhospital health facility, or died in the ED. Patients who were treated in the ED and then admitted to the same or a different hospital for inpatient services were not included, because they represent a different type of patient (e.g., in terms of condition severity or treatment needs). The earlier HCUP Statistical Briefs that focused on inpatient stays included admitted patients who were initially treated in the ED. For this report, ED super-utilizers were defined on the basis of a consistent cut-off rule of approximately 2 standard deviations above the mean number of ED visits during 2014, applied to the statistical distribution specific to each payer and age group:
Findings Patient demographics and outcomes of ED visits among super-utilizers by payer, 2014 Table 1 presents patient demographic characteristics for ED visits among super-utilizers compared with other patients by payer in 2014. |
|
| Table 1. Demographic characteristics and outcomes for ED visits among super-utilizersa by payer, 13 States, 2014 | ||||||||
| Characteristicb | Medicare aged 65+ years | Medicare aged 1-64 years | Private insurance aged 1-64 years | Medicaid aged 1-64 years | ||||
|---|---|---|---|---|---|---|---|---|
| Super-utilizersa | Other patients | Super-utilizersa | Other patients | Super-utilizersa | Other patients | Super-utilizersa | Other patients | |
| Total number of ED visits, thousands | 606 | 3,144 | 568 | 1,602 | 937 | 7,996 | 1,762 | 8,766 |
| Mean age, years | 76.7 | 76.8 | 46.3 | 48.6 | 34.9 | 34.2 | 32.3 | 24.2 |
| Female, % | 59.7 | 60.0 | 57.0 | 55.9 | 66.2 | 56.5 | 69.3 | 61.8 |
| Number of chronic conditions, % | ||||||||
| 0 | 27.1 | 31.2 | 39.3 | 44.3 | 63.7 | 72.7 | 60.7 | 76.6 |
| 1-2 | 39.6 | 42.1 | 40.6 | 39.0 | 31.0 | 24.0 | 32.0 | 20.6 |
| 3+ | 33.3 | 26.7 | 20.1 | 16.7 | 5.3 | 3.3 | 7.3 | 2.7 |
| Discharge disposition,c % | ||||||||
| Discharged to home or self-care | 92.0 | 92.7 | 93.8 | 94.3 | 96.7 | 97.5 | 95.4 | 97.1 |
| Transfer to a nonhospital facility | 4.7 | 3.9 | 2.2 | 2.3 | 0.8 | 0.7 | 1.1 | 0.8 |
| Home healthcare | 1.2 | 0.9 | 0.3 | 0.3 | 0.1 | 0.1 | 0.1 | 0.1 |
| Against medical advice | 1.7 | 1.5 | 3.5 | 2.6 | 2.2 | 1.5 | 3.2 | 1.9 |
| Died in hospital | 0.1 | 0.8 | 0.0 | 0.3 | 0.0 | 0.1 | 0.0 | 0.0 |
| Abbreviations: ED, emergency department Note: ED visits comprise patients who were treated in the ED and then released from the ED, transferred to another nonhospital health facility, or died in the ED. Patients who were treated in the ED and then admitted to a hospital for inpatient services were not included. a Super-utilizers are patients aged 1-64 years covered by Medicare or Medicaid with six or more ED visits and privately insured patients aged 1-64 years or Medicare patients aged 65 years and older with four or more ED visits in 2014 (approximately 2 standard deviations above the mean within each payer group). b Patient demographic characteristics are reported across ED visits, not across patients. All ED visits for a patient in 2014 are included in the analysis. The payer-age group classification was identified on the basis of the patient's first ED visit during the year and applied to all subsequent visits. The statistics presented on patient age, sex, and chronic conditions were identified on the basis of each individual ED visit. c Missing, invalid, or unknown discharge dispositions are not reported in the table. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), State Emergency Department Databases (SEDD) from 13 States, 2014 | ||||||||
Resource use and types of ED visits for super-utilizers by payer, 2014 Table 2 presents information on the number of ED visits, ED charges, and types of ED visits among super-utilizers compared with other patients by payer in 2014. Figure 1 presents the share of total ED visits and ED charges that were attributable to super-utilizers by payer in 2014. |
| Table 2. Resource use and types of ED visits for super-utilizersa by payer, 13 States, 2014 | ||||||||
| Resource use, outcome | Medicare aged 65+ years | Medicare aged 1-64 years | Private insurance aged 1-64 years | Medicaid aged 1-64 years | ||||
|---|---|---|---|---|---|---|---|---|
| Super-utilizersa | Other patients | Super-utilizersa | Other patients | Super-utilizersa | Other patients | Super-utilizersa | Other patients | |
| Mean number of ED visits per year | 5.4 | 1.3 | 10.2 | 1.9 | 6.1 | 1.4 | 9.5 | 1.8 |
| Average total charge per ED visit,b $ | 4,200 | 5,000 | 3,400 | 3,800 | 3,200 | 3,300 | 2,700 | 2,300 |
| Aggregate ED charges,b $ billions | 2.6 | 15.6 | 1.9 | 6.0 | 3.0 | 26.4 | 4.6 | 19.9 |
| Type of ED visit, % | ||||||||
| Medical | 82.2 | 76.7 | 79.9 | 76.8 | 78.6 | 68.9 | 74.2 | 72.3 |
| Mental health | 3.7 | 1.9 | 8.2 | 5.4 | 4.4 | 3.2 | 7.0 | 3.5 |
| Injury | 14.1 | 21.4 | 11.2 | 17.0 | 12.0 | 24.8 | 11.5 | 18.4 |
| Maternal/neonatal | 0.0 | 0.0 | 0.7 | 0.7 | 4.9 | 3.1 | 7.4 | 5.8 |
| Abbreviations: ED, emergency department Note: ED visits comprise patients who were treated in the ED and then released from the ED, transferred to another nonhospital health facility, or died in the ED. Patients who were treated in the ED and then admitted to a hospital for inpatient services were not included. a Super-utilizers are patients aged 1-64 years covered by Medicare or Medicaid with six or more ED visits and privately insured patients aged 1-64 years or Medicare patients aged 65 years and older with four or more ED visits in 2014 (approximately 2 standard deviations above the mean within each payer group). b Charges represent the total charges for ED services. ED costs are not presented because ED cost-to-charge ratios are not available. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), State Emergency Department Databases (SEDD) from 13 States, 2014 | ||||||||
|
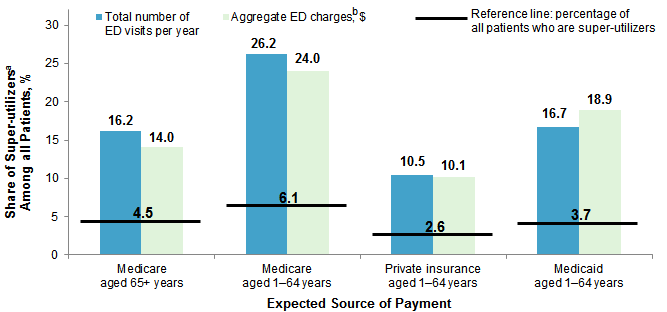
Figure 1. Share of ED super-utilizersa among all patients by payer, 13 States, 2014
Abbreviations: ED, emergency department Bar chart that shows the share of super-utilizers among all patients by payer in 2014. Medicare aged 65+ years: total number of emergency department visits per year: 16.2%; aggregate emergency department charges: 14.0%; percentage of all patients who are super-utilizers: 4.5%. Medicare aged 1-64 years: total number of emergency department visits per year: 26.2%; aggregate emergency department charges: 24.0%; percentage of all patients who are super-utilizers: 6.1%. Private insurance, aged 1-64 years: total number of emergency department visits per year: 10.5%; aggregate emergency department charges: 10.1%; percentage of all patients who are super-utilizers: 2.6%. Medicaid aged 1-64 years: total number of emergency department visits per year: 16.7%; aggregate emergency department charges: 18.9%; percentage of all patients who are super-utilizers: 3.7%.
|
Common first-listed diagnoses for ED visits among super-utilizers by payer, 2014 Table 3 lists the five most common first-listed diagnoses for ED visits among super-utilizers by payer in 2014. The share of ED visits attributed to super-utilizers by payer also is provided for each of the top five first-listed diagnoses. |
| Table 3. Top five first-listed diagnoses for ED visits among super-utilizersa by payer, 13 States, 2014 | ||||||||
| First-listed diagnosisa | Rank of diagnosis based on ED visits by payer | Share of ED visits attributed to super-utilizers by payer, % | ||||||
|---|---|---|---|---|---|---|---|---|
| Medicare 65+ years | Medicare 1-64 years | Private 1-64 years | Medicaid 1-64 years | Medicare 65+ years | Medicare 1-64 years | Private 1-64 years | Medicaid 1-64 years |
|
| All ED visits | - | - | - | - | 16 | 26 | 11 | 17 |
| Nonspecific chest pain | 1 | 2 | 5 | 16 | 28 | 10 | ||
| Superficial injury; contusion | 2 | 14 | ||||||
| Abdominal pain | 3 | 1 | 1 | 1 | 21 | 34 | 15 | 24 |
| Urinary tract infections | 4 | 19 | ||||||
| Spondylosis; intervertebral disc disorders; other back problems | 5 | 3 | 3 | 3 | 18 | 29 | 13 | 25 |
| Headache; including migraine | 4 | 2 | 5 | 40 | 19 | 25 | ||
| Sprains and strains | 5 | 4 | 22 | 7 | ||||
| Other complications of pregnancy | 2 | 22 | ||||||
| Other upper respiratory infections | 4 | 10 | ||||||
| Abbreviations: ED, emergency department Note: ED visits comprise patients who were treated in the ED and then released from the ED, transferred to another hospital or health facility, or died in the ED. Patients who were treated in the ED and then admitted to the same hospital for inpatient services were not included. a Super-utilizers are patients aged 1-64 years covered by Medicare or Medicaid with six or more ED visits and privately insured patients aged 1-64 years or Medicare patients aged 65 years and older with four or more ED visits in 2014 (approximately 2 standard deviations above the mean within each payer group). b Diagnoses are from the Clinical Classifications Software (CCS) categories based on International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnoses. All ED visits for a patient in 2014 are included in the analysis. First-listed diagnoses were identified on the basis of each individual ED visit. Source: Agency for Healthcare Research and Quality (AHRQ), Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project (HCUP), State Emergency Department Databases (SEDD) from 13 States, 2014 | ||||||||
Data Source The estimates in this Statistical Brief are based upon data from the Healthcare Cost and Utilization Project (HCUP) 2014 State Emergency Department Databases (SEDD) from 13 States: Florida, Georgia, Iowa, Maryland, Missouri, Nebraska, Nevada, New York, South Carolina, South Dakota, Tennessee, Vermont, and Wisconsin. Only patients aged 1 year and older were included in the analysis. Verified patient linkage numbers tend to be less reliable and less complete for patients less than 1 year old, which makes it difficult to track multiple ED visits. Definitions Diagnoses, ICD-9-CM, and Clinical Classifications Software (CCS) The first-listed diagnosis is the condition, symptom, or problem identified in the medical record to be chiefly responsible for the emergency department services provided. ICD-9-CM is the International Classification of Diseases, Ninth Revision, Clinical Modification, which assigns numeric codes to diagnoses. There are approximately 14,000 ICD-9-CM diagnosis codes. CCS categorizes ICD-9-CM diagnosis codes into a manageable number of clinically meaningful categories.5 This clinical grouper makes it easier to quickly understand patterns of diagnoses. CCS categories identified as Other typically are not reported; these categories include miscellaneous, otherwise unclassifiable diagnoses that may be difficult to interpret as a group. Types of hospitals included in HCUP State Emergency Department Databases This analysis used State Emergency Department Databases (SEDD) limited to data from community hospitals with a hospital-owned emergency department. Community hospitals are defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons). Community hospitals include specialty, pediatric, public, and academic medical hospitals. Excluded for this analysis are long-term care facilities such as rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Unit of analysis The unit of analysis is the emergency department (ED) encounter, not a person or patient. This means that a person who is seen in the ED multiple times in 1 year will be counted each time as a separate encounter in the ED. In this Statistical Brief, ED visits comprise patients who are treated in the ED and are not admitted to the same hospital or transferred to another acute care hospital for further treatment. Patients may be released home from the ED, be referred to home healthcare, go to another type of long-term or intermediate care facility (nursing home or psychiatric treatment facility), leave against medical advice, die, or be released alive but the destination is unknown. ED visit use in the year determined which category a patient was assigned to for all of their visits (e.g., Medicare super-utilizers aged 1-64 years). The payer-age group for the patient was defined by the first ED visit in the year. For example, a Medicare patient who was 64 years old for a January ED visit and 65 years old for a September ED visit would be included in the Medicare aged 1-64 years group. After each patient was assigned to a payer-age group, the total number of ED visits in 2014 was determined for each unique patient. Using the distribution of total number of ED visits within each payer-age group, the cut-off for super-utilizers was defined as approximately 2 standard deviations above the average total number of ED visits. The assignment of the payer-age group and whether the patient qualified as a super-utilizer in that group was then added to each ED visit record for that patient. The analysis considered all ED visits in the year. Charges Charges represent what the hospital billed for the ED visit. ED total charges reflect the amount the hospital charged for the ED services, excluding professional (physician) fees. For the purposes of this Statistical Brief, charges are reported to the nearest hundred dollars. Payer Payer is the expected payer for the hospital stay. To make coding uniform across all HCUP data sources, payer combines detailed categories into general groups:
For the purpose of this analysis, the expected payer designation was assigned on the basis of a hierarchy of Medicare, Medicaid, and then privately insured. Medicare was identified on the basis of a payer code of Medicare as a primary, secondary, or tertiary payer regardless of any other reported payers. This means that individuals who were dually eligible for Medicare and Medicaid were categorized as Medicare. If not already assigned to Medicare, Medicaid was identified on the basis of a payer code of Medicaid as a primary, secondary, or tertiary payer regardless of any other reported payers. If not already assigned to Medicare or Medicaid, private insurance was identified on the basis of a payer code of private insurance as a primary, secondary, or tertiary payer. Number of chronic conditions per patient All diagnoses on all records were determined to be either chronic or nonchronic. The definition of chronic conditions was based on the Chronic Condition Indicator, which can be found at https://www.hcup-us.ahrq.gov/toolssoftware/chronic/chronic.jsp. Discharge status Discharge status reflects the disposition of the patient at discharge from the ED and includes the following six categories: routine (to home or self-care); transfer to another acute care hospital; transfer to a nonhospital facility (including skilled nursing facility, intermediate care, and another type of facility such as a nursing home); home healthcare; against medical advice (AMA); or died in the hospital. Transfers to another acute care hospital were excluded from this analysis to ensure that ED visits for transferred patients were not double counted. Type of ED visit Coding criteria for the four ED visit types are based on ICD-9-CM and CCS categories.6 Each visit was assigned to a single ED visit type, hierarchically, based on the following order: maternal/neonatal, mental health, injury, and medical. About HCUP The Healthcare Cost and Utilization Project (HCUP, pronounced "H-Cup") is a family of healthcare databases and related software tools and products developed through a Federal-State-Industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). HCUP databases bring together the data collection efforts of State data organizations, hospital associations, and private data organizations (HCUP Partners) and the Federal government to create a national information resource of encounter-level healthcare data. HCUP includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, medical practice patterns, access to healthcare programs, and outcomes of treatments at the national, State, and local market levels. HCUP would not be possible without the contributions of the following data collection Partners from across the United States: Alaska Department of Health and Social Services Alaska State Hospital and Nursing Home Association Arizona Department of Health Services Arkansas Department of Health California Office of Statewide Health Planning and Development Colorado Hospital Association Connecticut Hospital Association District of Columbia Hospital Association Florida Agency for Health Care Administration Georgia Hospital Association Hawaii Health Information Corporation Illinois Department of Public Health Indiana Hospital Association Iowa Hospital Association Kansas Hospital Association Kentucky Cabinet for Health and Family Services Louisiana Department of Health Maine Health Data Organization Maryland Health Services Cost Review Commission Massachusetts Center for Health Information and Analysis Michigan Health & Hospital Association Minnesota Hospital Association Mississippi State Department of Health Missouri Hospital Industry Data Institute Montana MHA - An Association of Montana Health Care Providers Nebraska Hospital Association Nevada Department of Health and Human Services New Hampshire Department of Health & Human Services New Jersey Department of Health New Mexico Department of Health New York State Department of Health North Carolina Department of Health and Human Services North Dakota (data provided by the Minnesota Hospital Association) Ohio Hospital Association Oklahoma State Department of Health Oregon Association of Hospitals and Health Systems Oregon Office of Health Analytics Pennsylvania Health Care Cost Containment Council Rhode Island Department of Health South Carolina Revenue and Fiscal Affairs Office South Dakota Association of Healthcare Organizations Tennessee Hospital Association Texas Department of State Health Services Utah Department of Health Vermont Association of Hospitals and Health Systems Virginia Health Information Washington State Department of Health West Virginia Health Care Authority Wisconsin Department of Health Services Wyoming Hospital Association About Statistical Briefs HCUP Statistical Briefs are descriptive summary reports presenting statistics on hospital inpatient and emergency department use and costs, quality of care, access to care, medical conditions, procedures, patient populations, and other topics. The reports use HCUP administrative healthcare data. About the SEDD The HCUP State Emergency Department Databases (SEDD) include information from hospital-owned emergency departments (EDs) from data organizations participating in HCUP, translated into a uniform format to facilitate multistate comparisons and analyses. The SEDD capture information on ED visits that do not result in an admission to the same hospital (i.e., patients who are treated in the ED and then discharged, transferred to another hospital, left against medical advice, or died). The SEDD contain a core set of clinical and nonclinical information on all patients, including individuals covered by Medicare, Medicaid, or private insurance, as well as those who are uninsured. The SEDD can be used to investigate questions unique to one State, to compare data from two or more States, to conduct market-area variation analyses, and to identify State-specific trends in injury surveillance, emerging infections, and other conditions treated in the ED. For More Information For other information on readmissions and revisits, including super-utilizers, refer to the HCUP Statistical Briefs located at http://www.hcup-us.ahrq.gov/reports/statbriefs/sb_readmission.jsp. For additional HCUP statistics, visit:
For a detailed description of HCUP and more information on the design of the State Emergency Department Databases (SEDD), please refer to the following database documentation: Agency for Healthcare Research and Quality. Overview of the State Emergency Department Databases (SEDD). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated June 2016. http://www.hcup-us.ahrq.gov/seddoverview.jsp. Accessed January 5, 2017. Suggested Citation Jiang HJ (AHRQ), Weiss AJ (IBM Watson Health), Barrett ML (M.L. Barrett, Inc.). Characteristics of Emergency Department Visits for Super-Utilizers by Payer, 2014. HCUP Statistical Brief #221. February 2017. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb221-Super-Utilizer-ED-Visits-Payer-2014.pdf. Acknowledgments The authors would like to acknowledge the contributions of Minya Sheng of IBM Watson Health. *** AHRQ welcomes questions and comments from readers of this publication who are interested in obtaining more information about access, cost, use, financing, and quality of healthcare in the United States. We also invite you to tell us how you are using this Statistical Brief and other HCUP data and tools, and to share suggestions on how HCUP products might be enhanced to further meet your needs. Please e-mail us at hcup@ahrq.gov or send a letter to the address below:Sharon Arnold, Ph.D., Acting Director Center for Delivery, Organization, and Markets Agency for Healthcare Research and Quality 5600 Fishers Lane Rockville, MD 20857 This Statistical Brief was posted online on February 28, 2017. 1 Jiang HJ, Barrett ML, Sheng M. Characteristics of Hospital Stays for Nonelderly Medicaid Super-Utilizers, 2012. HCUP Statistical Brief #184. November 2014. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb184-Hospital-Stays-Medicaid-Super-Utilizers-2012.pdf. Accessed October 6, 2016. 2 Jiang HJ, Weiss AJ, Barrett ML, Sheng M. Characteristics of Hospital Stays for Super-Utilizers by Payer, 2012. HCUP Statistical Brief #190. May 2015. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb190-Hospital-Stays-Super-Utilizers-Payer-2012.pdf. Accessed September 27, 2016. 3 Ibid. 4 Ibid. 5 Agency for Healthcare Research and Quality. HCUP Clinical Classifications Software (CCS). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated June 2015. http://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp. Accessed February 17, 2016. 6 ED visit types were adapted from the hospital service line variable used in the HCUP State Inpatient Databases (SID). Diagnosis-related groups (DRGs), which are used to distinguish surgical and medical stays with inpatient data, are not available with ED visit data; all ED visits that did not fall into one of the other ED visit types (maternal/neonatal, mental health, or injury) were categorized as medical. Agency for Healthcare Research and Quality. Central Distributor SID: Description of Data Elements-SERVICELINE. Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality. Updated August 2008. https://www.hcup-us.ahrq.gov/db/vars/siddistnote.jsp?var=serviceline. Accessed January 27, 2017. |